Mini-Open Anterior Retroperitoneal Lumbar Interbody Fusion: Oblique Lateral Interbody Fusion for Lumbar Spinal Degeneration Disease
- Affiliations
-
- 1Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba, Japan. sohtori@faculty.chiba-u.jp
- KMID: 2366348
- DOI: http://doi.org/10.3349/ymj.2015.56.4.1051
Abstract
- PURPOSE
Surgery for lumbar spinal degeneration disease is widely performed. While posterior decompression and fusion are popular, anterior lumbar interbody fusion (ALIF) is also used for treatment. Extreme lateral interbody fusion (XLIF) is commonly used for noninvasive ALIF; however, several complications, such as spinal nerve and psoas muscle injury, have been reported. In the current study, we examined the clinical efficacy and complications of oblique lateral interbody fusion (OLIF) for lumbar spinal degeneration disease.
MATERIALS AND METHODS
Thirty-five patients with degenerated spondylolisthesis, discogenic pain, and kyphoscoliosis were examined. All patients underwent OLIF surgery (using a cage and bone graft from the iliac crest) with or without posterior decompression, without real-time electromyography monitoring. Posterior screws were used in all patients. Visual analog scale (VAS) score and Oswestry Disability Index (ODI) were evaluated before and 6 months after surgery. Surgical complications were also evaluated.
RESULTS
Pain scores significantly improved after surgery, compared to those before surgery (p<0.05). There was no patient who underwent revision surgery. There was no spinal nerve, major vessel, peritoneal, or urinary injury. Few patients showed symptoms from psoas invasion.
CONCLUSION
OLIF surgery produced good surgical results without any major complication.
Keyword
MeSH Terms
Figure
-
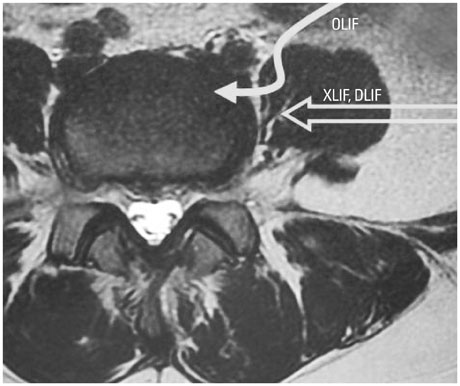
Fig. 1 Approaches to OLIF, XLIF, and DLIF. DLIF and XLIF present a lower risk of vessel or peritoneal injury but an increased risk of injury to spinal nerves or psoas muscles. OLIF is an anterior-psoas approach. OLIF, oblique lateral interbody fusion; XLIF, extreme lateral interbody fusion; DLIF, direct lateral interbody fusion.
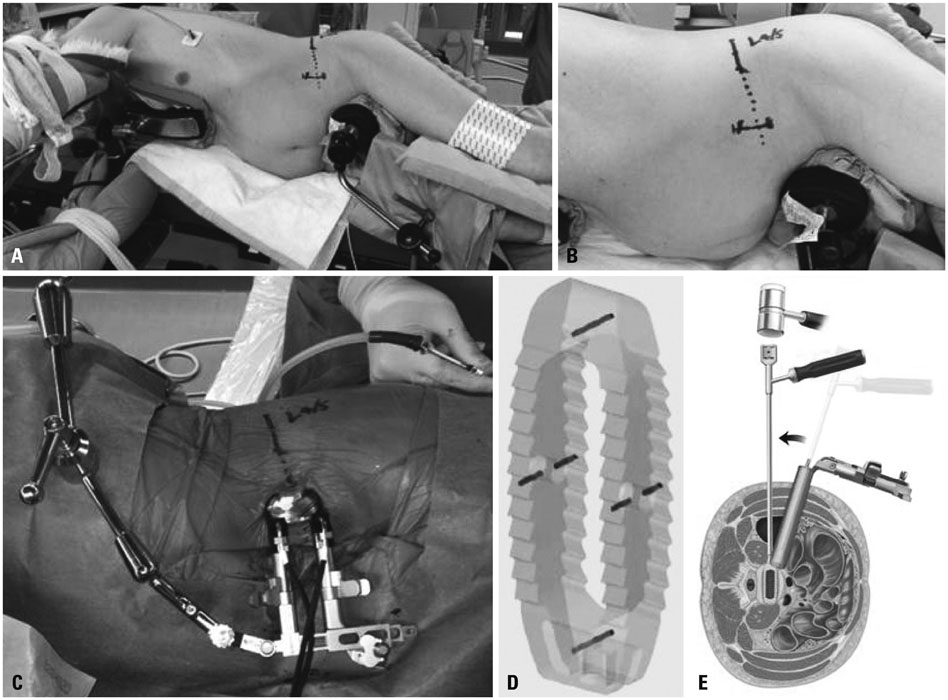
Fig. 2 (A) Skin marking to check the disc level using a C-arm X-ray imager. The skin incision was made 6 to 10 cm anterior to the mid portion of the disc. (A and B) Longitudinal incision from 3 to 4 cm is recommended. (C) Retractor for OLIF. (D) Clydesdale Spinal System cage filled with autologous bone is implanted. (E) Implantation technique. Implantation starts from a lateral oblique direction; finally the cage is inserted from a true lateral direction. OLIF, oblique lateral interbody fusion.

Fig. 3 A 68-year-old woman showing spondylolisthetic degeneration at L4. MRI (A and B) and myelography (C) showing spondylolisthetic degeneration at L4 and spinal stenosis at L4-5. After surgery (OLIF and percutaneous pedicle screws without posterior decompression), disc height, spondylolisthesis, and stenosis improved on myelography (D). OLIF, oblique lateral interbody fusion.

Fig. 4 (A) A 74-year-old woman showing kyphosis and discogenic pain. X-ray image showing severe kyphosis from L3 to L5. (B) MRI showing disc degeneration and Modic type 1 and 3 change at L4 and L5 vertebrae. (C) Surgery (OLIF and percutaneous pedicle screws without posterior decompression) improved the kyphosis. OLIF, oblique lateral interbody fusion.
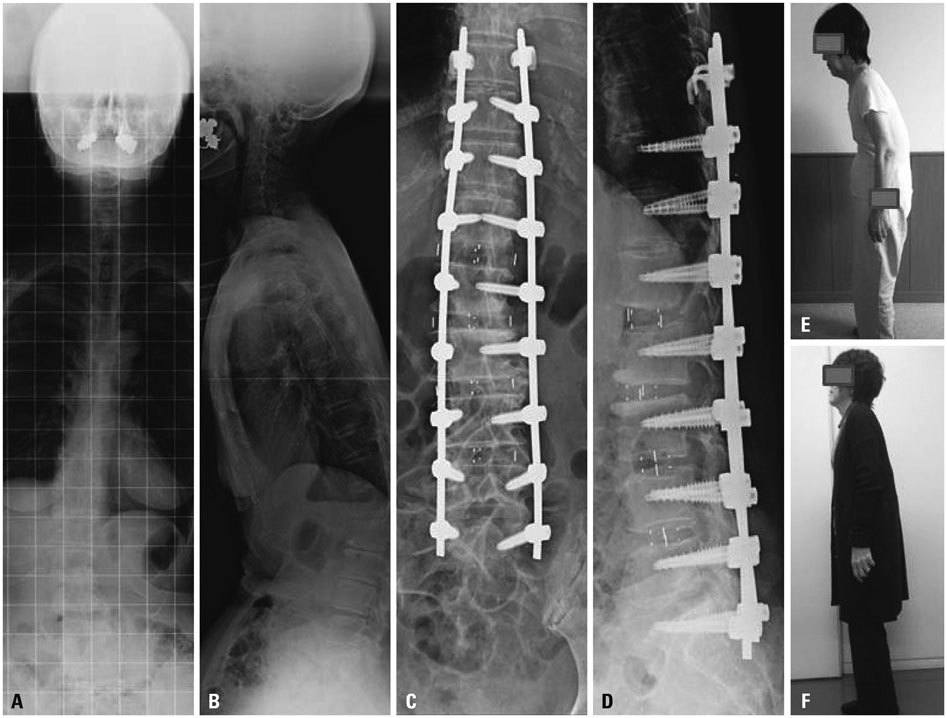
Fig. 5 (A and B) A 78-year-old woman showing kyphoscoliosis. X-ray images showing kyphoscoliosis. (C and D) Surgery (OLIF and percutaneous pedicle screws without posterior decompression) improved the kyphoscoliosis. (E) Photo before surgery. (F) Photo after surgery. OLIF, oblique lateral interbody fusion.
Cited by 3 articles
-
Effect of Sagittal Balance on Risk of Falling after Lateral Lumbar Interbody Fusion Surgery Combined with Posterior Surgery
Byung Ho Lee, Jae-Ho Yang, Hak-Sun Kim, Kyung-Soo Suk, Hwan-Mo Lee, Jin-Oh Park, Seong-Hwan Moon
Yonsei Med J. 2017;58(6):1177-1185. doi: 10.3349/ymj.2017.58.6.1177.Learning Curve and Complications Experience of Oblique Lateral Interbody Fusion : A Single-Center 143 Consecutive Cases
Bu Kwang Oh, Dong Wuk Son, Su Hun Lee, Jun Seok Lee, Soon Ki Sung, Sang Weon Lee, Geun Sung Song
J Korean Neurosurg Soc. 2021;64(3):447-459. doi: 10.3340/jkns.2020.0342.Do Obliquity and Position of the Oblique Lumbar Interbody Fusion Cage Influence the Degree of Indirect Decompression of Foraminal Stenosis?
Akaworn Mahatthanatrakul, Vit Kotheeranurak, Guang-Xun Lin, Jung-Woo Hur, Ho-Jung Chung, Yadhu K Lokanath, Boonserm Pakdeenit, Jin-Sung Kim
J Korean Neurosurg Soc. 2022;65(1):74-83. doi: 10.3340/jkns.2021.0105.
Reference
-
1. Chastain CA, Eck JC, Hodges SD, Humphreys SC, Levi P. Transforaminal lumbar interbody fusion: a retrospective study of long-term pain relief and fusion outcomes. Orthopedics. 2007; 30:389–392.
Article2. Gill K, Blumenthal SL. Posterior lumbar interbody fusion. A 2-year follow-up of 238 patients. Acta Orthop Scand Suppl. 1993; 251:108–110.
Article3. Ishihara H, Osada R, Kanamori M, Kawaguchi Y, Ohmori K, Kimura T, et al. Minimum 10-year follow-up study of anterior lumbar interbody fusion for isthmic spondylolisthesis. J Spinal Disord. 2001; 14:91–99.
Article4. Takahashi K, Kitahara H, Yamagata M, Murakami M, Takata K, Miyamoto K, et al. Long-term results of anterior interbody fusion for treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1990; 15:1211–1215.
Article5. Tiusanen H, Seitsalo S, Osterman K, Soini J. Retrograde ejaculation after anterior interbody lumbar fusion. Eur Spine J. 1995; 4:339–342.
Article6. Okuda S, Miyauchi A, Oda T, Haku T, Yamamoto T, Iwasaki M. Surgical complications of posterior lumbar interbody fusion with total facetectomy in 251 patients. J Neurosurg Spine. 2006; 4:304–309.
Article7. Ozgur BM, Aryan HE, Pimenta L, Taylor WR. Extreme Lateral Interbody Fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006; 6:435–443.
Article8. Pimenta L. Lateral endoscopic transpsoas retroperitoneal approach for lumbar spine surgery. In : Paper presented at the VIII Brazilian Spine Society Meeting; May 2001; Belo Horizonte, Minas Gerais, Brazil.9. Bergey DL, Villavicencio AT, Goldstein T, Regan JJ. Endoscopic lateral transpsoas approach to the lumbar spine. Spine (Phila Pa 1976). 2004; 29:1681–1688.
Article10. Cummock MD, Vanni S, Levi AD, Yu Y, Wang MY. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J Neurosurg Spine. 2011; 15:11–18.
Article11. Silvestre C, Mac-Thiong JM, Hilmi R, Roussouly P. Complications and Morbidities of Mini-open Anterior Retroperitoneal Lumbar Interbody Fusion: Oblique Lumbar Interbody Fusion in 179 Patients. Asian Spine J. 2012; 6:89–97.
Article12. Ohtori S, Koshi T, Yamashita M, Takaso M, Yamauchi K, Inoue G, et al. Single-level instrumented posterolateral fusion versus non-instrumented anterior interbody fusion for lumbar spondylolisthesis: a prospective study with a 2-year follow-up. J Orthop Sci. 2011; 16:352–358.
Article13. Schofferman J, Slosar P, Reynolds J, Goldthwaite N, Koestler M. A prospective randomized comparison of 270 degrees fusions to 360 degrees fusions (circumferential fusions). Spine (Phila Pa 1976). 2001; 26:E207–E212.14. Kitchel SH, Matteri RE. Prospective randomized evaluation of PLIF in degenerative spondylolisthesis patients over 60 years old. Curr Concepts Rev. 2002.15. Videbaek TS, Christensen FB, Soegaard R, Hansen ES, Høy K, Helmig P, et al. Circumferential fusion improves outcome in comparison with instrumented posterolateral fusion: long-term results of a randomized clinical trial. Spine (Phila Pa 1976). 2006; 31:2875–2880.
Article16. Acosta FL, Liu J, Slimack N, Moller D, Fessler R, Koski T. Changes in coronal and sagittal plane alignment following minimally invasive direct lateral interbody fusion for the treatment of degenerative lumbar disease in adults: a radiographic study. J Neurosurg Spine. 2011; 15:92–96.
Article17. Anand N, Baron EM, Thaiyananthan G, Khalsa K, Goldstein TB. Minimally invasive multilevel percutaneous correction and fusion for adult lumbar degenerative scoliosis: a technique and feasibility study. J Spinal Disord Tech. 2008; 21:459–467.
Article18. Anand N, Rosemann R, Khalsa B, Baron EM. Mid-term to long-term clinical and functional outcomes of minimally invasive correction and fusion for adults with scoliosis. Neurosurg Focus. 2010; 28:E6.
Article19. Youssef JA, McAfee PC, Patty CA, Raley E, DeBauche S, Shucosky E, et al. Minimally invasive surgery: lateral approach interbody fusion: results and review. Spine (Phila Pa 1976). 2010; 35:26 Suppl. S302–S311.20. Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements. Spine (Phila Pa 1976). 2010; 35:26 Suppl. S331–S337.
Article21. Marchi L, Abdala N, Oliveira L, Amaral R, Coutinho E, Pimenta L. Radiographic and clinical evaluation of cage subsidence after stand-alone lateral interbody fusion. J Neurosurg Spine. 2013; 19:110–118.
Article22. Davis TT, Bae HW, Mok JM, Rasouli A, Delamarter RB. Lumbar plexus anatomy within the psoas muscle: implications for the transpsoas lateral approach to the L4-L5 disc. J Bone Joint Surg Am. 2011; 93:1482–1487.
Article23. Uribe JS, Arredondo N, Dakwar E, Vale FL. Defining the safe working zones using the minimally invasive lateral retroperitoneal transpsoas approach: an anatomical study. J Neurosurg Spine. 2010; 13:260–266.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Lateral Lumbar Interbody Fusion: Indications, Outcomes and Complications
- Minimally Invasive Strategy for Uniportal Full-Endoscopic Transforaminal Lumbar Interbody Fusion Using a Large Cage Utilized in Oblique Lumbar Interbody Fusion
- Pearls and Pitfalls of Oblique Lateral Interbody Fusion: A Comprehensive Narrative Review
- Morphometric Analysis of the Ureter with Respect to Lateral Lumbar Interbody Fusion Using Contrast-Enhanced Computed Tomography
- Clinical Comparison between Decompression and Posterior Lumbar Interbody Fusion in Chronic Lower Back Pain Involving Degenerative Disc Disease and Spinal Stenosis
