Immune-Checkpoint Inhibitors in the Era of Precision Medicine: What Radiologists Should Know
- Affiliations
-
- 1Department of Radiology, Brigham and Women's Hospital and Dana Farber Cancer Institute, Boston, MA 02215, USA. mbraschi@partners.org
- 2Department of Medical Oncology and Medicine, Dana Farber Cancer Institue, Boston, MA 02215, USA.
- KMID: 2468121
- DOI: http://doi.org/10.3348/kjr.2017.18.1.42
Abstract
- Over the past five years immune-checkpoint inhibitors have dramatically changed the therapeutic landscape of advanced solid and hematologic malignancies. The currently approved immune-checkpoint inhibitors include antibodies to cytotoxic T-lymphocyte antigen-4, programmed cell death (PD-1), and programmed cell death ligand (PD-L1 and PD-L2). Response to immune-checkpoint inhibitors is evaluated on imaging using the immune-related response criteria. Activation of immune system results in a unique toxicity profile termed immune-related adverse events. This article will review the molecular mechanism, clinical applications, imaging of immune-related response patterns and adverse events associated with immune-checkpoint inhibitors.
MeSH Terms
-
Antibodies, Monoclonal/adverse effects/*therapeutic use
Antineoplastic Agents/adverse effects/*therapeutic use
B7-H1 Antigen/immunology
CTLA-4 Antigen/immunology
Humans
Immunotherapy/adverse effects/*methods
Neoplasms/*diagnostic imaging/immunology/*therapy
Precision Medicine/methods
Programmed Cell Death 1 Receptor/immunology
Antibodies, Monoclonal
Antineoplastic Agents
B7-H1 Antigen
CTLA-4 Antigen
Programmed Cell Death 1 Receptor
Figure
-

Fig. 1 62-year-old male with history of ocular melanoma metastatic to liver. A, B. Contrast enhanced coronal abdominal CT image shows single solid hepatic metastasis (black arrow, A); lung parenchyma is normal. C, D. After 8 weeks of treatment with combination therapy Ipilimumab/Nivolumab, patient presents to emergency department complaining of shortness of breath. While contrast enhanced coronal abdominal CT image shows decreased size and density of hepatic metastasis (black arrow, C), suggesting response to treatment, new lung consolidative opacities are concerning for drug pneumonitis (black arrows, D).
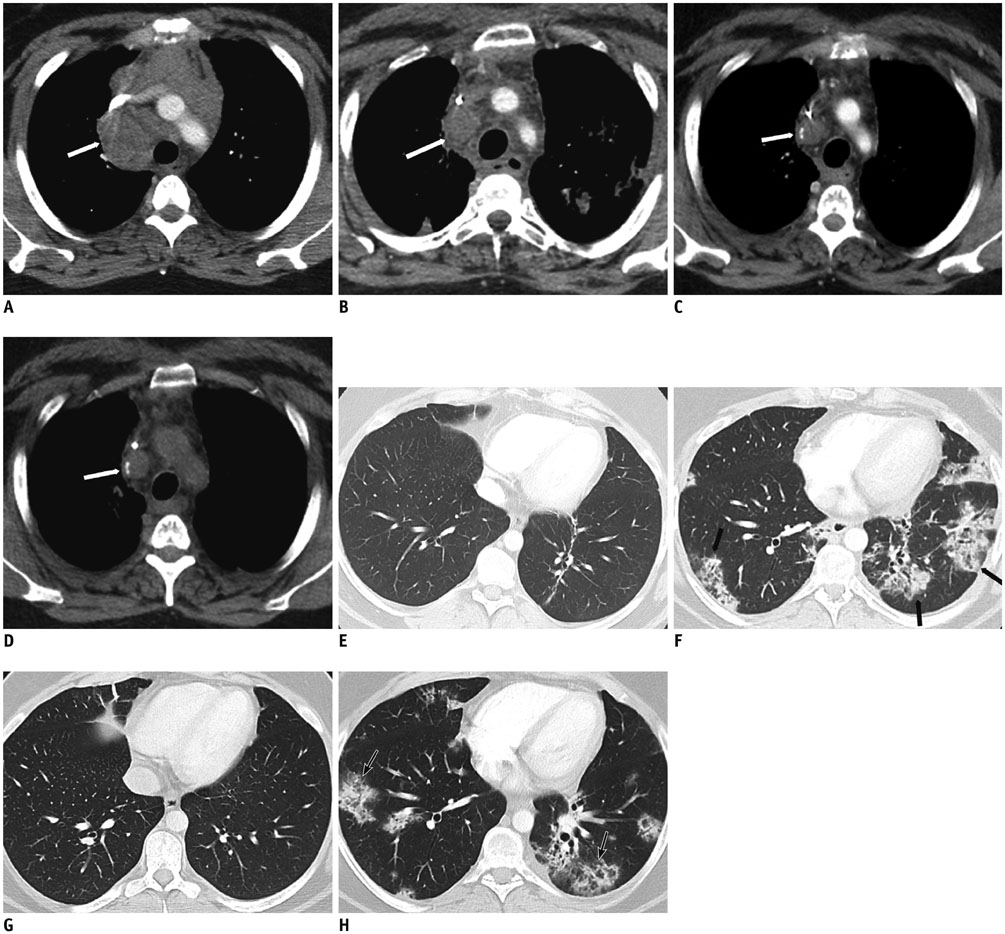
Fig. 2 33-year-old woman with history of Hodgkin’s lymphoma. A, E. Axial contrast enhanced CT image of mediastinum shows bulky mediastinal adenopathy (white arrow, A); lung parenchyma is normal. B, F. After 12 weeks of treatment with Nivolumab, while mediastinal lymph nodes have significantly decreased (white arrow, B), new parenchymal patchy bilateral opacities suggest drug pneumonitis (black arrows, F). C, G. Nivolumab was stopped, high dose therapy with corticosteroid initiated. After 4 weeks of steroid, axial CT image of lung parenchyma demonstrates resolution of pneumonitis, while mediastinal disease continues to decrease (white arrow). D, H. After steroid taper, while mediastinal adenopathy has not significantly changed (white arrow), axial chest CT in lung window shows recurrent pneumonitis (black arrows).

Fig. 3 73-year-old gentleman with history of recurrent squamous cell lung cancer. A, D. Axial contrast-enhanced CT image of mediastinum shows mediastinal adenopathy (white arrows, A); coronal abdominal image is unremarkable. B, E. After 4 weeks of treatment with Nivolumab, while mediastinal lymph nodes have significantly decreased (white arrow, B), visualized colon is hyperemic and fluid filled, suggesting colitis (black arrows, E). C, F. Nivolumab was stopped, high dose therapy with corticosteroid initiated. After 8 weeks, restaging contrast-enhanced abdominal CT shows resolution of colitis, but there has been significant increased in size of mediastinal adenopathy (white arrows, C).
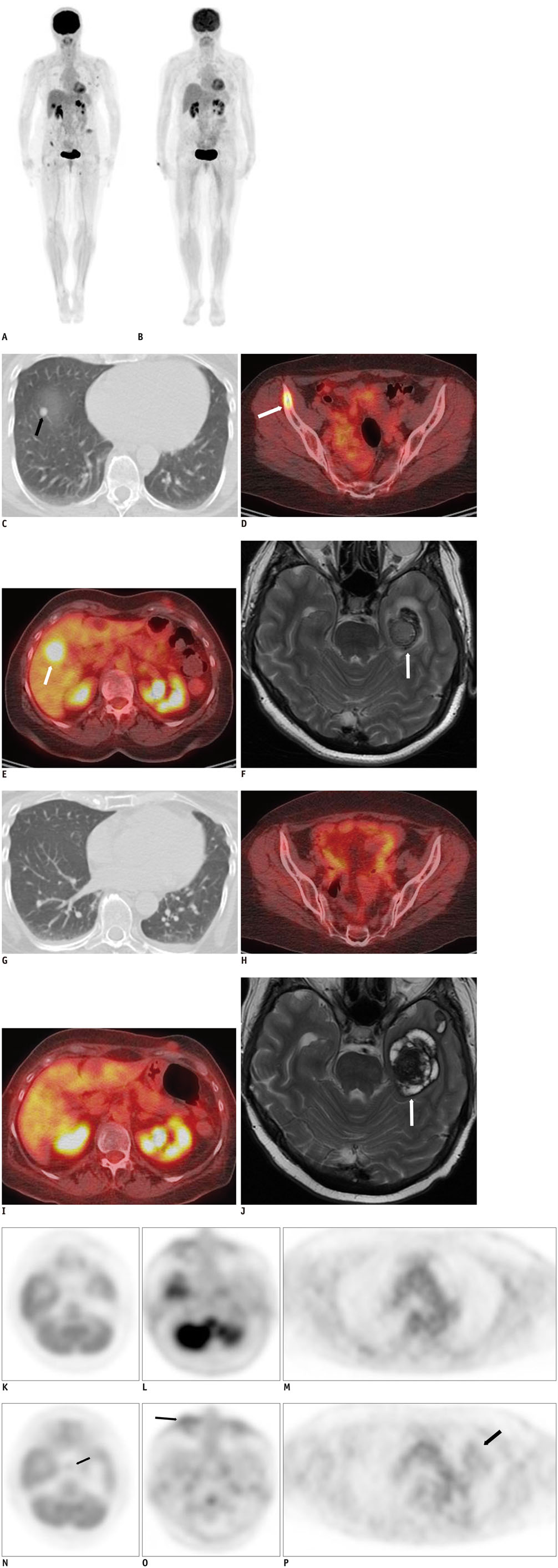
Fig. 4 59-year-old female with history of left arm melanoma, metastatic to lung, bones, liver brain and subcutaneous tissue, before and after 12 weeks of treatment with Ipilimumab. A. Whole body MIP F-FDG PET/CT image at baseline demonstrates tracer uptake within lung, bones, liver and subcutaneous tissue, suggesting widespread metastatic disease. B. Whole body MIP F-FDG PET/CT image after 12 weeks of treatment with Ipilimumab demonstrates interval resolution of tracer avidity at sites of metastases. F-FDG = fludeoxyglucose, MIP = maximum intensity projection, PET = positron emission tomography C-F. Axial CT image in lung window, fused PET/CT images of pelvis and liver, contrast enhanced T2 weighted MRI image of brain demonstrate right lower lobe nodule (black arrow, C), right iliac bone (white arrow, D), right liver (white arrow, E) and left temporal lobe metastases (white arrow, F). F-FDG = fludeoxyglucose, MIP = maximum intensity projection, PET = positron emission tomography G-J. Restaging imaging at 12 weeks after induction treatment with Ipilimumab show significant decrease of lung nodule, significant decrease uptake of right iliac bone lesion, of liver metastasis and decreased enhancement of brain metastasis (white arrow), suggesting response to treatment. K-M. Axial PET image of brain at level of hypophysis, mid face and mid thorax before treatment show physiologic tracer uptake. N-P. Restaging PET images at 12 weeks after induction treatment with Ipilimumab show interval increased uptake within hypophysis (black arrow, N), in region of palpebrae (black arrow, O) and left lung parenchyma (black arrow, P), which suggest drug associated hypophysitis, blepharoconjunctivitis and pneumonitis. F-FDG = fludeoxyglucose, MIP = maximum intensity projection, PET = positron emission tomography
Reference
-
1. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010; 363:711–723.2. Rosenberg SA. Adoptive immunotherapy of cancer: accomplishments and prospects. Cancer Treat Rep. 1984; 68:233–255.3. Jiang T, Zhou C, Ren S. Role of IL-2 in cancer immunotherapy. Oncoimmunology. 2016; 5:e1163462.4. Yoo S, Choi SY, You D, Kim CS. New drugs in prostate cancer. Prostate Int. 2016; 4:37–42.5. Chen Y, Liu D. Chimeric antigen receptor (CAR)-directed adoptive immunotherapy: a new era in targeted cancer therapy. Stem Cell Investig. 2014; 1:2.6. Freeman GJ, Long AJ, Iwai Y, Bourque K, Chernova T, Nishimura H, et al. Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J Exp Med. 2000; 192:1027–1034.7. Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science. 1996; 271:1734–1736.8. Brunet JF, Denizot F, Luciani MF, Roux-Dosseto M, Suzan M, Mattei MG, et al. A new member of the immunoglobulin superfamily--CTLA-4. Nature. 1987; 328:267–270.9. Freeman GJ, Gribben JG, Boussiotis VA, Ng JW, Restivo VA Jr, Lombard LA, et al. Cloning of B7-2: a CTLA-4 counter-receptor that costimulates human T cell proliferation. Science. 1993; 262:909–911.10. Calabrò L, Morra A, Fonsatti E, Cutaia O, Fazio C, Annesi D, et al. Efficacy and safety of an intensified schedule of tremelimumab for chemotherapy-resistant malignant mesothelioma: an open-label, single-arm, phase 2 study. Lancet Respir Med. 2015; 3:301–309.11. Hodi FS, Fisher DE. Adoptive transfer of antigen-specific CD4+ T cells in the treatment of metastatic melanoma. Nat Clin Pract Oncol. 2008; 5:696–697.12. Wolchok JD, Neyns B, Linette G, Negrier S, Lutzky J, Thomas L, et al. Ipilimumab monotherapy in patients with pretreated advanced melanoma: a randomised, double-blind, multicentre, phase 2, dose-ranging study. Lancet Oncol. 2010; 11:155–164.13. Ishida Y, Agata Y, Shibahara K, Honjo T. Induced expression of PD-1, a novel member of the immunoglobulin gene superfamily, upon programmed cell death. EMBO J. 1992; 11:3887–3895.14. Topalian SL, Sznol M, McDermott DF, Kluger HM, Carvajal RD, Sharfman WH, et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J Clin Oncol. 2014; 32:1020–1030.15. Robert C, Ribas A, Wolchok JD, Hodi FS, Hamid O, Kefford R, et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet. 2014; 384:1109–1117.16. Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, et al. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med. 2013; 369:134–144.17. Choueiri TK, Fishman MN, Escudier B, McDermott DF, Drake CG, Kluger H, et al. Immunomodulatory activity of nivolumab in metastatic renal cell carcinoma. Clin Cancer Res. 2016; 05. 11. [Epub]. DOI: 10.1158/1078-0432.CCR-15-2839.18. Gettinger S, Rizvi NA, Chow LQ, Borghaei H, Brahmer J, Ready N, et al. Nivolumab monotherapy for first-line treatment of advanced non-small-cell lung cancer. J Clin Oncol. 2016; 34:2980–2987.19. Armand P. Immune checkpoint blockade in hematologic malignancies. Blood. 2015; 125:3393–3400.20. Ansell SM, Lesokhin AM, Borrello I, Halwani A, Scott EC, Gutierrez M, et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin’s lymphoma. N Engl J Med. 2015; 372:311–319.21. Perales MA, Sauter CS, Armand P. Fast cars and no brakes: autologous stem cell transplantation as a platform for novel immunotherapies. Biol Blood Marrow Transplant. 2016; 22:17–22.22. Roemer MG, Advani RH, Ligon AH, Natkunam Y, Redd RA, Homer H, et al. PD-L1 and PD-L2 genetic alterations define classical Hodgkin lymphoma and predict outcome. J Clin Oncol. 2016; 34:2690–2697.23. Lesokhin AM, Ansell SM, Armand P, Scott EC, Halwani A, Gutierrez M, et al. Nivolumab in patients with relapsed or refractory hematologic malignancy: preliminary results of a phase Ib Study. J Clin Oncol. 2016; 34:2698–2704.24. Armand P. Checkpoint blockade in lymphoma. Hematology Am Soc Hematol Educ Program. 2015; 2015:69–73.25. Davids MS, Kim HT, Bachireddy P, Costello C, Liguori R, Savell A, et al. Ipilimumab for patients with relapse after allogeneic transplantation. N Engl J Med. 2016; 375:143–153.26. Armand P, Shipp MA, Ribrag V, Michot JM, Zinzani PL, Kuruvilla J, et al. Programmed death-1 blockade with pembrolizumab in patients with classical Hodgkin lymphoma after brentuximab vedotin failure. J Clin Oncol. 2016; 06. 27. [Epub]. DOI: 10.1200/JCO.2016.67.3467.27. Rosenberg JE, Hoffman-Censits J, Powles T, van der Heijden MS, Balar AV, Necchi A, et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm, multicentre, phase 2 trial. Lancet. 2016; 387:1909–1920.28. Weber J, Thompson JA, Hamid O, Minor D, Amin A, Ron I, et al. A randomized, double-blind, placebo-controlled, phase II study comparing the tolerability and efficacy of ipilimumab administered with or without prophylactic budesonide in patients with unresectable stage III or IV melanoma. Clin Cancer Res. 2009; 15:5591–5598.29. Wolchok JD, Kluger H, Callahan MK, Postow MA, Rizvi NA, Lesokhin AM, et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013; 369:122–133.30. Wolchok JD, Hoos A, O’Day S, Weber JS, Hamid O, Lebbé C, et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009; 15:7412–7420.31. O’Regan KN, Jagannathan JP, Ramaiya N, Hodi FS. Radiologic aspects of immune-related tumor response criteria and patterns of immune-related adverse events in patients undergoing ipilimumab therapy. AJR Am J Roentgenol. 2011; 197:W241–W246.32. Kwak JJ, Tirumani SH, Van den Abbeele AD, Koo PJ, Jacene HA. Cancer immunotherapy: imaging assessment of novel treatment response patterns and immune-related adverse events. Radiographics. 2015; 35:424–437.33. Nishino M, Tirumani SH, Ramaiya NH, Hodi FS. Cancer immunotherapy and immune-related response assessment: the role of radiologists in the new arena of cancer treatment. Eur J Radiol. 2015; 84:1259–1268.34. Nishino M, Giobbie-Hurder A, Ramaiya NH, Hodi FS. Response assessment in metastatic melanoma treated with ipilimumab and bevacizumab: CT tumor size and density as markers for response and outcome. J Immunother Cancer. 2014; 2:40.35. Nishino M, Gargano M, Suda M, Ramaiya NH, Hodi FS. Optimizing immune-related tumor response assessment: does reducing the number of lesions impact response assessment in melanoma patients treated with ipilimumab? J Immunother Cancer. 2014; 2:17.36. Nishino M, Giobbie-Hurder A, Gargano M, Suda M, Ramaiya NH, Hodi FS. Developing a common language for tumor response to immunotherapy: immune-related response criteria using unidimensional measurements. Clin Cancer Res. 2013; 19:3936–3943.37. Nishino M. Immune-related response evaluations during immune-checkpoint inhibitor therapy: establishing a “common language” for the new arena of cancer treatment. J Immunother Cancer. 2016; 4:30.38. Erasmus JJ, Gladish GW, Broemeling L, Sabloff BS, Truong MT, Herbst RS, et al. Interobserver and intraobserver variability in measurement of non-small-cell carcinoma lung lesions: implications for assessment of tumor response. J Clin Oncol. 2003; 21:2574–2582.39. Nishino M, Guo M, Jackman DM, DiPiro PJ, Yap JT, Ho TK, et al. CT tumor volume measurement in advanced non-small-cell lung cancer: performance characteristics of an emerging clinical tool. Acad Radiol. 2011; 18:54–62.40. Zhao B, James LP, Moskowitz CS, Guo P, Ginsberg MS, Lefkowitz RA, et al. Evaluating variability in tumor measurements from same-day repeat CT scans of patients with non-small cell lung cancer. Radiology. 2009; 252:263–272.41. Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer treatment. Cancer. 1981; 47:207–214.42. Zhao B, Tan Y, Bell DJ, Marley SE, Guo P, Mann H, et al. Exploring intra- and inter-reader variability in uni-dimensional, bi-dimensional, and volumetric measurements of solid tumors on CT scans reconstructed at different slice intervals. Eur J Radiol. 2013; 82:959–968.43. Nishino M, Hatabu H, Johnson BE, McLoud TC. State of the art: response assessment in lung cancer in the era of genomic medicine. Radiology. 2014; 271:6–27.44. Bohnsack O, Ludajic K, Hoos A. Adaptation of the immune-related response criteria: irRECIST. Massachusetts: ESMO;2014. p. Abstract 4958.45. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000; 92:205–216.46. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009; 45:228–247.47. Nishino M, Jagannathan JP, Ramaiya NH, Van den Abbeele AD. Revised RECIST guideline version 1.1: What oncologists want to know and what radiologists need to know. AJR Am J Roentgenol. 2010; 195:281–289.48. Nishino M, Jagannathan JP, Krajewski KM, O’Regan K, Hatabu H, Shapiro G, et al. Personalized tumor response assessment in the era of molecular medicine: cancer-specific and therapy-specific response criteria to complement pitfalls of RECIST. AJR Am J Roentgenol. 2012; 198:737–745.49. Hodi FS, Hwu WJ, Kefford R, Weber JS, Daud A, Hamid O, et al. Evaluation of immune-related response criteria and RECIST v1.1 in patients with advanced melanoma treated with pembrolizumab. J Clin Oncol. 2016; 34:1510–1517.50. Tirumani SH, Ramaiya NH, Keraliya A, Bailey ND, Ott PA, Hodi FS, et al. Radiographic profiling of immune-related adverse events in advanced melanoma patients treated with ipilimumab. Cancer Immunol Res. 2015; 3:1185–1192.51. Nishino M, Chambers ES, Chong CR, Ramaiya NH, Gray SW, Marcoux JP, et al. Anti-PD-1 inhibitor-related pneumonitis in non-small cell lung cancer. Cancer Immunol Res. 2016; 4:289–293.52. Nishino M, Sholl LM, Hodi FS, Hatabu H, Ramaiya NH. Anti-PD-1-related pneumonitis during cancer immunotherapy. N Engl J Med. 2015; 373:288–290.53. Bronstein Y, Ng CS, Hwu P, Hwu WJ. Radiologic manifestations of immune-related adverse events in patients with metastatic melanoma undergoing anti-CTLA-4 antibody therapy. AJR Am J Roentgenol. 2011; 197:W992–W1000.54. Kim KW, Ramaiya NH, Krajewski KM, Shinagare AB, Howard SA, Jagannathan JP, et al. Ipilimumab-associated colitis: CT findings. AJR Am J Roentgenol. 2013; 200:W468–W474.55. Min JH, Lee HY, Lim H, Ahn MJ, Park K, Chung MP, et al. Drug-induced interstitial lung disease in tyrosine kinase inhibitor therapy for non-small cell lung cancer: a review on current insight. Cancer Chemother Pharmacol. 2011; 68:1099–1109.56. Kim KW, Ramaiya NH, Krajewski KM, Jagannathan JP, Tirumani SH, Srivastava A, et al. Ipilimumab associated hepatitis: imaging and clinicopathologic findings. Invest New Drugs. 2013; 31:1071–1077.57. González-Rodríguez E, Rodríguez-Abreu D. Spanish Group for Cancer Immuno-Biotherapy (GETICA). Immune Checkpoint Inhibitors: Review and Management of Endocrine Adverse Events. Oncologist. 2016; 21:804–816.58. Carpenter KJ, Murtagh RD, Lilienfeld H, Weber J, Murtagh FR. Ipilimumab-induced hypophysitis: MR imaging findings. AJNR Am J Neuroradiol. 2009; 30:1751–1753.59. Eckert A, Schoeffler A, Dalle S, Phan A, Kiakouama L, Thomas L. Anti-CTLA4 monoclonal antibody induced sarcoidosis in a metastatic melanoma patient. Dermatology. 2009; 218:69–70.60. Berthod G, Lazor R, Letovanec I, Romano E, Noirez L, Mazza Stalder J, et al. Pulmonary sarcoid-like granulomatosis induced by ipilimumab. J Clin Oncol. 2012; 30:e156–e159.61. Hunter G, Voll C, Robinson CA. Autoimmune inflammatory myopathy after treatment with ipilimumab. Can J Neurol Sci. 2009; 36:518–520.62. Weber JS, Kähler KC, Hauschild A. Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol. 2012; 30:2691–2697.63. Howard SA, Krajewski KM, Jagannathan JP, Braschi-Amirfarzan M, Tirumani SH, Shinagare AB, et al. A new look at toxicity in the era of precision oncology: imaging findings, their relationship with tumor response, and effect on metastasectomy. AJR Am J Roentgenol. 2016; 207:4–14.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of advanced urogenital cancers with immune checkpoint inhibitors
- Advances in immune checkpoint inhibitors for hepatocellular carcinoma
- Red Blood Cell Autoantibodies in Patients Treated with Immune Checkpoint Inhibitors
- Gut microbiome on immune checkpoint inhibitor therapy and consequent immune-related colitis: a review
- Current status of cancer immunotherapy with immune checkpoint inhibitors
