Follicular Bronchiolitis Mimicking Lung Cancer in a Patient with Primary Sjögren's Syndrome
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. yn35@snu.ac.kr
- 2Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- 3WCU Department of Molecular Medicine and Biopharmaceutical Sciences, Medical Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2451513
- DOI: http://doi.org/10.4078/jrd.2019.26.3.206
Abstract
- Follicular bronchiolitis (FB) is an uncommon pulmonary lymphoproliferative disorder that is characterized by the presence of peribronchiolar hyperplastic lymphoid follicles with reactive germinal centers. FB could be associated with systemic illnesses including immunodeficiency, infection, and autoimmune diseases. In Korea, a single case of FB with rheumatoid arthritis was recently described but there has been no report on FB associated with other rheumatic diseases. Herein, we describe the first case of FB presenting nodular ground-glass opacities (GGO), which mimicked lung cancer, in patients with primary Sjögren's syndrome (SS). The differential diagnosis of nodular GGO lesions should include FB although it is a rare manifestation in SS patients.
MeSH Terms
Figure
-

Figure 1 Serial follow-ups of chest computed tomography (CT). (A) Chest CT showed a nodular ground-glass opacity (GGO) lesion in the left upper lobe, 31 months prior to admission. (B) Seven months prior to admission, the longitudinal diameter of the nodular GGO lesion was slightly increased (from 13.5 to 15.0 mm over 24 months).

Figure 2 Chest computed tomography (CT) and positron emission tomography (PET)-CT images. (A) Matched CT and PET/CT scan slices demonstrated a 15 mm-sized lesion of nodular ground-glass opacities (GGO) without pathological uptake of 18F-fluorodeoxyglucose in the anterior segment of the left upper lobe. (B) Chest CT scan images revealed a new GGO nodule in the superior segment of the right lower lobe and the corresponding PET-CT slice showed the lesion with hypermetabolism (maximal standardized uptake value 2.1).
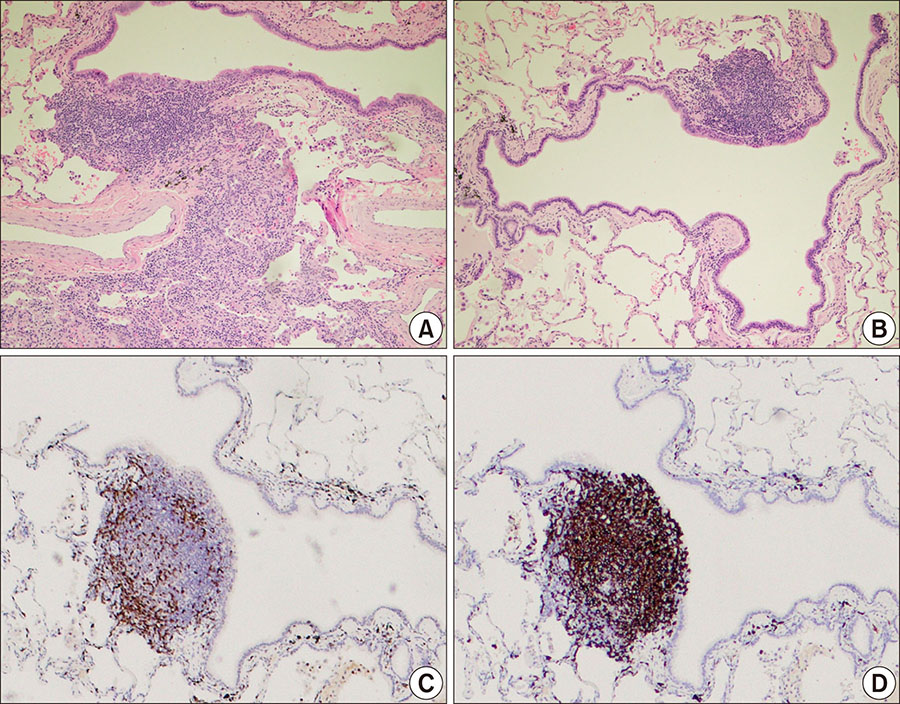
Figure 3 Pathology of lung biopsy specimen. In hematoxylin and eosin stained section, peribronchiolar lymphoid hyperplasia with polymorphous lymphoid populations was observed (A, ×100). Additionally, the destruction of peribronchial alveolar septa was not shown (B, ×100). Immunohistochemistry study for CD3 (C) and CD20 (D) showed that most mononuclear cells were nonmalignant B cells in the peribronchial follicular lymphoid hyperplasia (×40).
Reference
-
1. Mariette X, Criswell LA. Primary Sjögren's Syndrome. N Engl J Med. 2018; 378:931–939.2. Flament T, Bigot A, Chaigne B, Henique H, Diot E, Marchand-Adam S. Pulmonary manifestations of Sjögren's syndrome. Eur Respir Rev. 2016; 25:110–123.3. Tashtoush B, Okafor NC, Ramirez JF, Smolley L. Follicular bronchiolitis: a literature review. J Clin Diagn Res. 2015; 9:OE01–OE05.4. Pipavath SJ, Lynch DA, Cool C, Brown KK, Newell JD. Radiologic and pathologic features of bronchiolitis. AJR Am J Roentgenol. 2005; 185:354–363.5. Fortoul TI, Cano-Valle F, Oliva E, Barrios R. Follicular bronchiolitis in association with connective tissue diseases. Lung. 1985; 163:305–314.6. Lee YJ, Park JH, Cho GJ, Lee BC, Kim DS, Suh YL, et al. A case of follicular bronchitis/bronchiolitis. Korean J Med. 1993; 45:795–800.7. Lee JH, Choi M, Oh SS, Choi MR, Yang HJ, Lee KM, et al. Case of follicular bronchiolitis in rheumatoid arthritis. J Rheum Dis. 2016; 23:392–395.8. Hwangbo Y, Cha SI, Lee YH, Lee SY, Seo H, Oh S, et al. A case of multicentric castleman's disease presenting with follicular bronchiolitis. Tuberc Respir Dis (Seoul). 2013; 74:23–27.9. Kim MS, Lim SC, Kim YH, Na KJ, Kim KS, Kwon KY, et al. A case report of localized form of follicular bronchitis/bronchiolitis with fibrosis. Tuberc Respir Dis. 1998; 45:191–196.10. Jeong Y, Bang YH, Kim YK. Migrating persistent pulmonary consolidation in a child: a case of follicular bronchiolitis. Pediatr Pulmonol. 2017; 52:E22–E25.11. Ysamat Marfá R, Benito Ysamat A, Espejo Pérez S, Blanco Negredo M, Roldán Molina R. Lung disease associated with connective tissue disease. Radiologia. 2013; 55:107–117.12. Kim HJ, Kim KH, Hann HJ, Han S, Kim Y, Lee SH, et al. Incidence, mortality, and causes of death in physician-diagnosed primary Sjögren's syndrome in Korea: a nationwide, population-based study. Semin Arthritis Rheum. 2017; 47:222–227.13. Aerni MR, Vassallo R, Myers JL, Lindell RM, Ryu JH. Follicular bronchiolitis in surgical lung biopsies: clinical implications in 12 patients. Respir Med. 2008; 102:307–312.14. Howling SJ, Hansell DM, Wells AU, Nicholson AG, Flint JD, Müller NL. Follicular bronchiolitis: thin-section CT and histologic findings. Radiology. 1999; 212:637–642.15. Palm O, Garen T, Berge Enger T, Jensen JL, Lund MB, Aaløkken TM, et al. Clinical pulmonary involvement in primary Sjogren's syndrome: prevalence, quality of life and mortality--a retrospective study based on registry data. Rheumatology (Oxford). 2013; 52:173–179.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Treatment with Steroid and Hydrochloroquine of Thrombocytopenia in Primary Sjögren's Syndrome
- Longitudinal Changes of the European League Against Rheumatism Sjögren's Syndrome Patient Reported Index in Korean Patients with Primary Sjögren's Syndrome
- Motor dominant polyradiculopathy with Primary Sjögren's syndrome mimicking motor neuron disease
- A Case of Sjögren-Larsson Syndrome
- Rehabilitation using twin-stage method for a Sjögren's syndrome patient with severe discoloration and attrition on upper and lower anterior teeth
