Tuberc Respir Dis.
2019 Jul;82(3):234-241. 10.4046/trd.2018.0087.
Utility of Computed Tomography in a Differential Diagnosis for the Patients with an Initial Diagnosis of Chronic Obstructive Pulmonary Disease Exacerbation
- Affiliations
-
- 1Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. ymoh55@amc.seoul.kr
- 2Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. seojb@amc.seoul.kr
- KMID: 2450901
- DOI: http://doi.org/10.4046/trd.2018.0087
Abstract
- BACKGROUND
The utility of computed tomography (CT) in the differential diagnosis of patients with chronic obstructive pulmonary disease (COPD) exacerbation remains uncertain. However, due to the low cost associated with CT scan along with the impact of Koreas' health insurance system, there has been a rise in the number of CT scans in the patients with initial diagnosis of COPD exacerbations. Therefore, the utility of CT in the differential diagnosis was investigated to determine whether performing CT scans affect the clinical outcomes of the patients with an initial diagnosis of COPD exacerbation.
METHODS
This study involved 202 COPD patients hospitalized with an initial diagnosis of COPD exacerbation. We evaluated the change in diagnosis or treatment after performing a CT scan, and compared the clinical outcomes of patient groups with vs. without performing CT (non-CT group vs. CT group).
RESULTS
After performing CT, the diagnosis was changed for two (3.0%) while additional diagnoses were made for 27 of the 64 patients (42.1%). However, the treatment changed for only one (1.5%), and six patients (9.3%) received supplementary medication. There were no difference in the median length of hospital stay (8 [6-13] days vs. 8 [6-12] days, p=0.786) and intensive care unit care (14 [10.1%] vs. 11 [16.7%], p=0.236) between the CT and non-CT groups, respectively. These findings remained consistent even after the propensity score matching.
CONCLUSION
Utility of CT in patients with acute COPD exacerbation might not be helpful; therefore, we do not recommend chest CT scan as a routine initial diagnostic tool.
Keyword
MeSH Terms
Figure
-
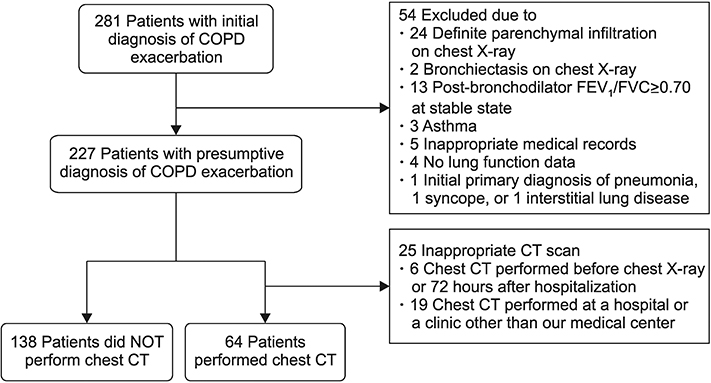
Figure 1 Flow of patient selection. We excluded the patients with bronchiectasis, history of asthma and the patients with definite parenchymal infiltration on the initial chest X-ray. In addition, we excluded the patients who performed chest computed tomography (CT) before the initial chest X-ray or 48 hours after hospitalization and also excluded the patients who performed chest CT at a hospital or a clinic other than our medical center. Initial diagnosis of chronic obstructive pulmonary disease (COPD) exacerbation is aggravated respiratory symptoms in COPD patients and defined as no definite infiltration on initial chest X-ray.
Reference
-
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of COPD. Global Initiative for Chronic Obstructive Lung Disease (GOLD);2016. p. 111.2. Abudagga A, Sun SX, Tan H, Solem CT. Exacerbations among chronic bronchitis patients treated with maintenance medications from a US managed care population: an administrative claims data analysis. Int J Chron Obstruct Pulmon Dis. 2013; 8:175–185.
Article3. Dixit D, Bridgeman MB, Andrews LB, Narayanan N, Radbel J, Parikh A, et al. Acute exacerbations of chronic obstructive pulmonary disease: diagnosis, management, and prevention in critically ill patients. Pharmacotherapy. 2015; 35:631–648.
Article4. Claessens YE, Debray MP, Tubach F, Brun AL, Rammaert B, Hausfater P, et al. Early chest computed tomography scan to assist diagnosis and guide treatment decision for suspected community-acquired pneumonia. Am J Respir Crit Care Med. 2015; 192:974–982.
Article5. Cardinale L, Priola AM, Moretti F, Volpicelli G. Effectiveness of chest radiography, lung ultrasound and thoracic computed tomography in the diagnosis of congestive heart failure. World J Radiol. 2014; 6:230–237.
Article6. Nagarsheth K, Kurek S. Ultrasound detection of pneumothorax compared with chest X-ray and computed tomography scan. Am Surg. 2011; 77:480–484.
Article7. Cheng T, Wan HY, Cheng QJ, Guo Y, Qian YR, Fan L, et al. Obvious emphysema on computed tomography during an acute exacerbation of chronic obstructive pulmonary disease predicts a poor prognosis. Intern Med J. 2015; 45:517–526.
Article8. Hackx M, Ghaye B, Coche E, Muylem AV, Gevenois PA. Severe COPD exacerbation: CT features. COPD. 2015; 12:38–45.
Article9. Cheng T, Wan H, Cheng Q, Guo YI, Qian Y, Fan L, et al. Computed tomography manifestation of acute exacerbation of chronic obstructive pulmonary disease: a pilot study. Exp Ther Med. 2016; 11:519–529.
Article10. Sogaard M, Madsen M, Lokke A, Hilberg O, Sorensen HT, Thomsen RW. Incidence and outcomes of patients hospitalized with COPD exacerbation with and without pneumonia. Int J Chron Obstruct Pulmon Dis. 2016; 11:455–465.11. Shapira-Rootman M, Beckerman M, Soimu U, Nachtigal A, Zeina AR. The prevalence of pulmonary embolism among patients suffering from acute exacerbations of chronic obstructive pulmonary disease. Emerg Radiol. 2015; 22:257–260.
Article12. Rizkallah J, Man SFP, Sin DD. Prevalence of pulmonary embolism in acute exacerbations of COPD: a systematic review and metaanalysis. Chest. 2009; 135:786–793.13. Rutschmann OT, Cornuz J, Poletti PA, Bridevaux PO, Hugli OW, Qanadli SD, et al. Should pulmonary embolism be suspected in exacerbation of chronic obstructive pulmonary disease? Thorax. 2007; 62:121–125.
Article14. Choi KJ, Cha SI, Shin KM, Lee J, Hwangbo Y, Yoo SS, et al. Prevalence and predictors of pulmonary embolism in Korean patients with exacerbation of chronic obstructive pulmonary disease. Respiration. 2013; 85:203–209.
Article15. Hartmann IJ, Hagen PJ, Melissant CF, Postmus PE, Prins MH. Diagnosing acute pulmonary embolism: effect of chronic obstructive pulmonary disease on the performance of D-dimer testing, ventilation/perfusion scintigraphy, spiral computed tomographic angiography, and conventional angiography. ANTELOPE Study Group. Advances in New Technologies Evaluating the Localization of Pulmonary Embolism. Am J Respir Crit Care Med. 2000; 162:2232–2237.16. Akpinar EE, Hosgun D, Doganay B, Atac GK, Gulhan M. Should the cut-off value of D-dimer be elevated to exclude pulmonary embolism in acute exacerbation of COPD? J Thorac Dis. 2013; 5:430–434.17. Garcia-Sanz MT, Canive-Gomez JC, Garcia-Couceiro N, Senin-Rial L, Alonso-Acuna S, Barreiro-Garcia A, et al. Factors associated with the incidence of serious adverse events in patients admitted with COPD acute exacerbation. Ir J Med Sci. 2017; 186:477–483.
Article18. Ramaraju K, Kaza AM, Balasubramanian N, Chandrasekaran S. Predicting healthcare utilization by patients admitted for COPD exacerbation. J Clin Diagn Res. 2016; 10:OC13–OC17.
Article19. Diamantea F, Kostikas K, Bartziokas K, Karakontaki F, Tsikrika S, Pouriki S, et al. Prediction of hospitalization stay in COPD exacerbations: the AECOPD-F score. Respir Care. 2014; 59:1679–1686.
Article20. Soltani A, Reid D, Wills K, Walters EH. Prospective outcomes in patients with acute exacerbations of chronic obstructive pulmonary disease presenting to hospital: a generalisable clinical audit. Intern Med J. 2015; 45:925–933.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Strongyloidiasis Masquerading as Exacerbation of Chronic Obstructive Pulmonary Disease
- The Clinical Study of Clarithromycin for the Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease
- Clinical Relevance of Bronchial Anthracofibrosis in Patients with Chronic Obstructive Pulmonary Disease Exacerbation
- Chronic Obstructive Pulmonary Disease: Respiratory Review of 2014
- The Relationship between Airway Inflammation and Exacerbation in Chronic Obstructive Pulmonary Disease
