Concurrence of Circumscribed Morphea and Segmental Vitiligo: A Case Report
- Affiliations
-
- 1Department of Dermatology, SMG-SNU Boramae Medical Center, Seoul, Korea. hsyoon79@gmail.com
- KMID: 2428928
- DOI: http://doi.org/10.5021/ad.2018.30.6.708
Abstract
- Although a few reports have noted the concurrent presentation of morphea and vitiligo at distinctly separate sites in the same patient, it is extremely rare that these two conditions occur at the same sites in a patient. We report the case of a 10-year-old Korean girl with morphea and vitiligo and those lesions occurred at the same sites and progressed simultaneously. An autoimmunity and a cutaneous mosaicism was considered to be involved in such an unique presentation as the pathogenesis is concerned.
Keyword
Figure
-

Fig. 1 (A) Multiple hypopigmented patches with small satellite lesions on the left upper arm, distributed along the T1 dermatome. (B) Indurated, atrophic, shiny areas at the center of hypopigmented patches.
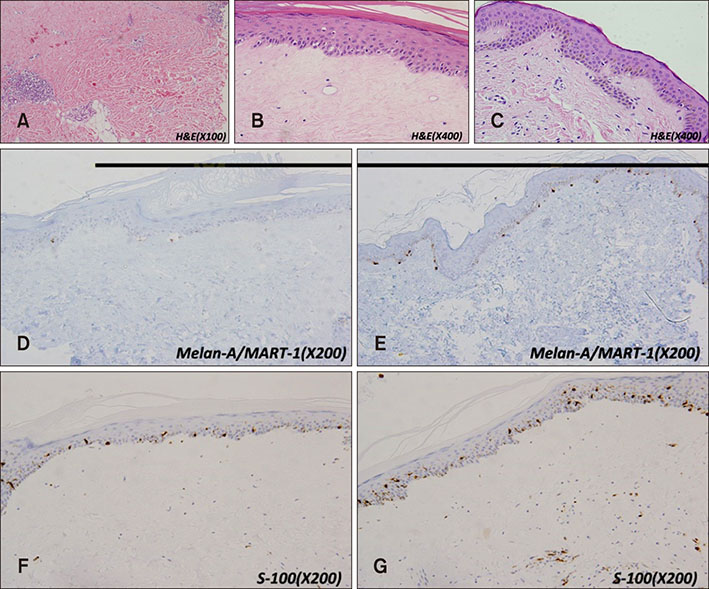
Fig. 2 (A) Biopsy from the depigmented lesion (H&E, ×100). Degenerated thickned dermal collagen bundles with focal dense lymphocytic infiltration. (B and C) Biopsy from the depigmented lesion (H&E, ×400) (B) showed a decresed basal pigmentation compared to adjacent normal peripheray (H&E, ×400) (C). Mild superficial perivascular lymphocytic infiltration was observed in the normal periphery (C). (D and E) Biopsy from the depigmented lesion (Melan-A/MART-1, ×200) (D) showed decreased Melan A positive melanocytes compared to adjacent normal periphery (Melan-A/MART-1, ×200) (E). (F and G) Biopsy from the depigmented lesion (S-100, ×200) (F) showed decreased S-100 positive melanocytes compared to adjacent normal periphery (S-100, ×200) (G).

Fig. 3 (A) Lesions before the treatment. (B) Lesions after 6 months of treatment. Improvement with repigmentation.
Reference
-
1. Bonifati C, Impara G, Morrone A, Pietrangeli A, Carducci M. Simultaneous occurrence of linear scleroderma and homolateral segmental vitiligo. J Eur Acad Dermatol Venereol. 2006; 20:63–65.
Article2. Yadav P, Garg T, Chander R, Nangia A. Segmental vitiligo with segmental morphea: an autoimmune link? Indian Dermatol Online J. 2014; 5:Suppl 1. S23–S25.
Article3. Finkelstein E, Amichai B, Metzker A. Coexistence of vitiligo and morphea: a case report and review of the literature. J Dermatol. 1995; 22:351–353.
Article4. Saihan EM, Peachey RD. Vitiligo and morphoea. Clin Exp Dermatol. 1979; 4:103–106.
Article5. Yorulmaz A, Kilic S, Artuz F, Kahraman E. Concomitant appearance of morphea and vitiligo in a patient with autoimmune thyroiditis. Postepy Dermatol Alergol. 2016; 33:314–316.
Article6. Dervis E, Acbay O, Barut G, Karaoglu A, Ersoy L. Association of vitiligo, morphea, and Hashimoto's thyroiditis. Int J Dermatol. 2004; 43:236–237.
Article7. Soylu S, Gul U, Gönül M, Kilic A, Cakmak SK, Demiriz M. An uncommon presentation of the co-existence of morphea and vitiligo in a patient with chronic hepatitis B virus infection: is there a possible association with autoimmunity? Am J Clin Dermatol. 2009; 10:336–338.
Article8. Bonilla-Abadia F, Muñoz-Buitrón E, Ochoa CD, Carrascal E, Cañas CA. A rare association of localized scleroderma type morphea, vitiligo, autoimmune hypothyroidism, pneumonitis, autoimmune thrombocytopenic purpura and central nervous system vasculitis. Case report. BMC Res Notes. 2012; 5:689.
Article9. Soma Y, Fujimoto M. Frontoparietal scleroderma (en coup de sabre) following Blaschko's lines. J Am Acad Dermatol. 1998; 38:366–368.
Article10. Gonzalez-Lopez MA, Drake M, Gonzalez-Vela MC, Armesto S, Llaca HF, Val-Bernal JF. Generalized morphea and primary biliary cirrhosis coexisting in a male patient. J Dermatol. 2006; 33:709–713.
Article11. Parra V, Driban N, Bassotti A. Localized morphea and myasthenia gravis. J Am Acad Dermatol. 2003; 49:E12.
Article12. Neucks SH, Moore TL, Lichtenstein JR, Baldassare AR, Weiss TD, Zuckner J. Localized scleroderma and idiopathic thrombocytopenia. J Rheumatol. 1980; 7:741–744.13. Arif T, Hassan I, Nisa N. Morphea and vitiligo-A very uncommon association. Our Dermatol Online. 2015; 6:232–234.
Article14. Takehara K, Sato S. Localized scleroderma is an autoimmune disorder. Rheumatology. 2005; 44:274–279.
Article15. Cunliffe WJ, Hall R, Newell DJ, Stevenson CJ. Vitiligo, thyroid disease and autoimmunity. Br J Dermatol. 1968; 80:135–139.
Article16. Dawber RP. Vitiligo in mature-onset diabetes mellitus. Br J Dermatol. 1968; 80:275–278.
Article17. Grunnet I, Howitz J, Reymann F, Schwartz M. Vitiligo and pernicious anemia. Arch Dermatol. 1970; 101:82–85.
Article18. Bor S, Feiwel M, Chanarin I. Vitiligo and its aetiological relationship to organ-specific autoimmune disease. Br J Dermatol. 1969; 81:83–88.
Article19. Bowcock AM, Fernandez-Vina M. Targeting skin: vitiligo and autoimmunity. J Invest Dermatol. 2012; 132:13–15.
Article20. Czajkowski R, Mecinska-Jundzill K. Current aspects of vitiligo genetics. Postepy Dermatol Alergol. 2014; 31:247–255.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Segmental Vitiligo
- Comparative Clinical Study of Segmental Vitiligo and Non-Segmental Vitiligo
- Classification and diagnosis of vitiligo
- The classification of segmental vitiligo on the face
- A Case of Simultaneous Occurrence of Vitiligo-like and Morphea-like Lesion in Recipient of Allogenic Bone Marrow Transplantation
