Multiple Myeloma in a Patient with Acromegaly
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. mskim@amc.seoul.kr
- 2Department of Laboratory Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2407113
- DOI: http://doi.org/10.3803/EnM.2015.30.1.110
Abstract
- Acromegaly is a slowly progressing condition resulting from excess growth hormone (GH), generally caused by a GH-secreting pituitary adenoma. Cancer is the third most common cause of mortality in patients with acromegaly, and insulin-like growth factor 1 (IGF-1) is known to influence tumor formation by increasing cell proliferation and inhibiting apoptosis. Multiple myeloma (MM) is a plasma cell neoplasm, and previous studies have suggested the possible role of IGF-1 in its development of MM. However, no cases of acromegaly accompanied with MM have been reported in Asia to date. We here report the case of a 58-year-old woman with acromegaly accompanied with MM who presented with longstanding acromegalic manifestations resulting from a GH-secreting pituitary adenoma and also exhibited anemia, a reversed albumin/globulin ratio, and plasmacytosis on bone marrow examination. Because IGF-1 has been suggested to play an important role in the development and progression of MM, the patient promptly underwent surgical removal of the pituitary adenoma via a transsphenoidal approach. Since there is currently no consensus on therapeutic guidelines and suggested prognosis for MM with acromegaly, long-term follow-up of such cases is needed.
MeSH Terms
-
Acromegaly*
Anemia
Apoptosis
Asia
Bone Marrow Examination
Cell Proliferation
Consensus
Female
Growth Hormone
Growth Hormone-Secreting Pituitary Adenoma
Humans
Insulin-Like Growth Factor I
Middle Aged
Mortality
Multiple Myeloma*
Neoplasms, Plasma Cell
Pituitary Neoplasms
Prognosis
Growth Hormone
Insulin-Like Growth Factor I
Figure
-

Fig. 1 (A) Physical examination of the patient revealed frontal bossing, thickened lips, and an enlarged nose. (B) Exaggerated frontal bossing (arrow) observed from the side. Disproportionately enlarged (acromegalic) hands (C) and feet (D) were also seen.
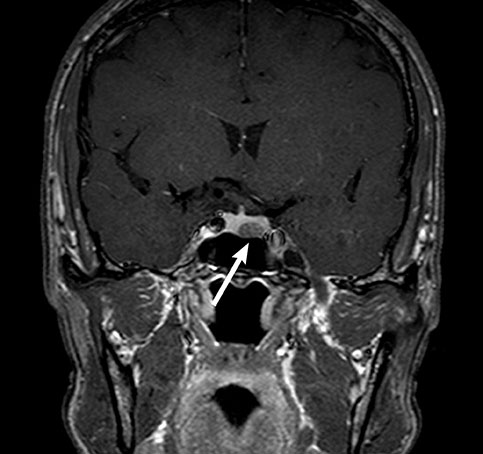
Fig. 2 A T1-weighted coronal magnetic resonance imaging of the sella turcica indicated a 10×6-mm hypointense, nonenhanced pituitary adenoma on the left side of the pituitary gland (arrow).
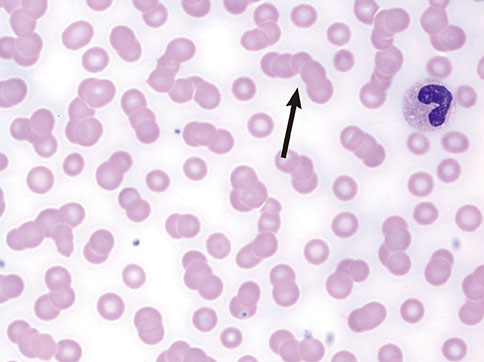
Fig. 3 Peripheral blood smear results revealed a red blood cell rouleaux formation (arrow; Wright stain, ×1,000).
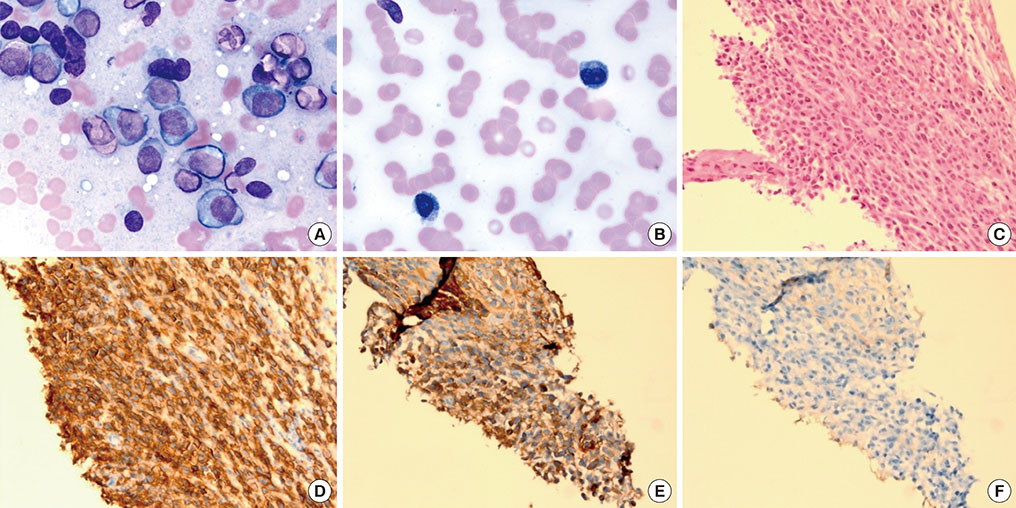
Fig. 4 (A) Neoplastic plasma cells in the bone marrow aspirate specimen (Wright stain, ×1,000). (B) Numerous clustered neoplastic plasma cells on a bone marrow touchprint slide. (C) Packed neoplastic plasma cells were prominent in a bone marrow biopsy specimen stained with H&E (×400). (D) CD138-positive neoplastic plasma cells in an immunohistochemically stained bone marrow biopsy specimen (×400). In an immunohistochemically stained bone marrow biopsy specimen, neoplastic cells were positive for λ light chain (E, ×400) and negative for κ light chain (F, ×400).
Reference
-
1. Nabarro JD. Acromegaly. Clin Endocrinol (Oxf). 1987; 26:481–512.2. Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am. 1999; 28:81–117.3. Orme SM, McNally RJ, Cartwright RA, Belchetz PE. Mortality and cancer incidence in acromegaly: a retrospective cohort study. United Kingdom Acromegaly Study Group. J Clin Endocrinol Metab. 1998; 83:2730–2734.4. Melmed S. Acromegaly and cancer: not a problem? J Clin Endocrinol Metab. 2001; 86:2929–2934.5. Hankinson SE, Willett WC, Colditz GA, Hunter DJ, Michaud DS, Deroo B, Rosner B, Speizer FE, Pollak M. Circulating concentrations of insulin-like growth factor-I and risk of breast cancer. Lancet. 1998; 351:1393–1396.6. Ma J, Pollak MN, Giovannucci E, Chan JM, Tao Y, Hennekens CH, Stampfer MJ. Prospective study of colorectal cancer risk in men and plasma levels of insulin-like growth factor (IGF)-I and IGF-binding protein-3. J Natl Cancer Inst. 1999; 91:620–625.7. Riedel DA, Pottern LM. The epidemiology of multiple myeloma. Hematol Oncol Clin North Am. 1992; 6:225–247.8. Murphy WJ, Rui H, Longo DL. Effects of growth hormone and prolactin immune development and function. Life Sci. 1995; 57:1–14.9. Georgii-Hemming P, Wiklund HJ, Ljunggren O, Nilsson K. Insulin-like growth factor I is a growth and survival factor in human multiple myeloma cell lines. Blood. 1996; 88:2250–2258.10. Kanazawa I, Yamaguchi T, Yamane Y, Murakami N, Kato Y, Sugimoto T. Acromegaly associated with monoclonal gammopathy of undetermined significance (MGUS). Endocr J. 2006; 53:687–691.11. Tucci A, Bonadonna S, Cattaneo C, Ungari M, Giustina A, Guiseppe R. Transformation of a MGUS to overt multiple myeloma: the possible role of a pituitary macroadenoma secreting high levels of insulin-like growth factor 1 (IGF-1). Leuk Lymphoma. 2003; 44:543–545.12. Barbosa FR, Vieira Neto L, Lima GA, Wildemberg LE, Portugal R, Gadelha MR. Hematologic neoplasias and acromegaly. Pituitary. 2011; 14:377–381.13. Hagg E, Asplund K, Holm J. Acromegaly and multiple myeloma. Ann Intern Med. 1988; 109:437–438.14. Ge NL, Rudikoff S. Insulin-like growth factor I is a dual effector of multiple myeloma cell growth. Blood. 2000; 96:2856–2861.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple myeloma
- Nonsecretory Multiple Myeloma associated with Immune Thrombocytopenia and Complicated by Malignant Ascites
- Acute Pancreatitis with Hypercalcemia as Initial Manifestation of Multiple Myeloma
- Continuous Multiple Vertebral Compression Fractures in Multiple Myeloma Patient
- Hereditary Aspect of Isolated Familial Acromegaly
