Acute Respiratory Failure due to Alveolar Hemorrhage after Exposure to Organic Dust
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, Korea.
- 2Department of Pathology, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, Korea. realrain7@gmail.com
- KMID: 2350928
- DOI: http://doi.org/10.4266/kjccm.2016.31.2.173
Abstract
- Diffuse alveolar hemorrhage (DAH) is associated with severe outcomes. We report a case of acute respiratory failure that required mechanical ventilation and was clinically and pathologically diagnosed as DAH related to exposure to organic dust. A 39-year-old man, who had visited a warehouse to grade beans for purchase, was referred to our hospital for impending respiratory failure. His initial radiographic examinations revealed diffuse bilateral ground-glass opacities in his lungs and bronchoalveolar lavage resulted in progressively bloodier returns, which is characteristic of DAH. He underwent bedside open lung biopsy of his right lower lobe in the intensive care unit. Biopsy results revealed DAH and organization with accumulation of hemosiderin-laden macrophages and a few fibroblastic foci. The patient was treated with empirical antibiotics and high-dose corticosteroids and successfully weaned from mechanical ventilation. DAH might be considered in the differential diagnosis of patients with acute respiratory failure after exposure to organic particles.
Keyword
MeSH Terms
Figure
-
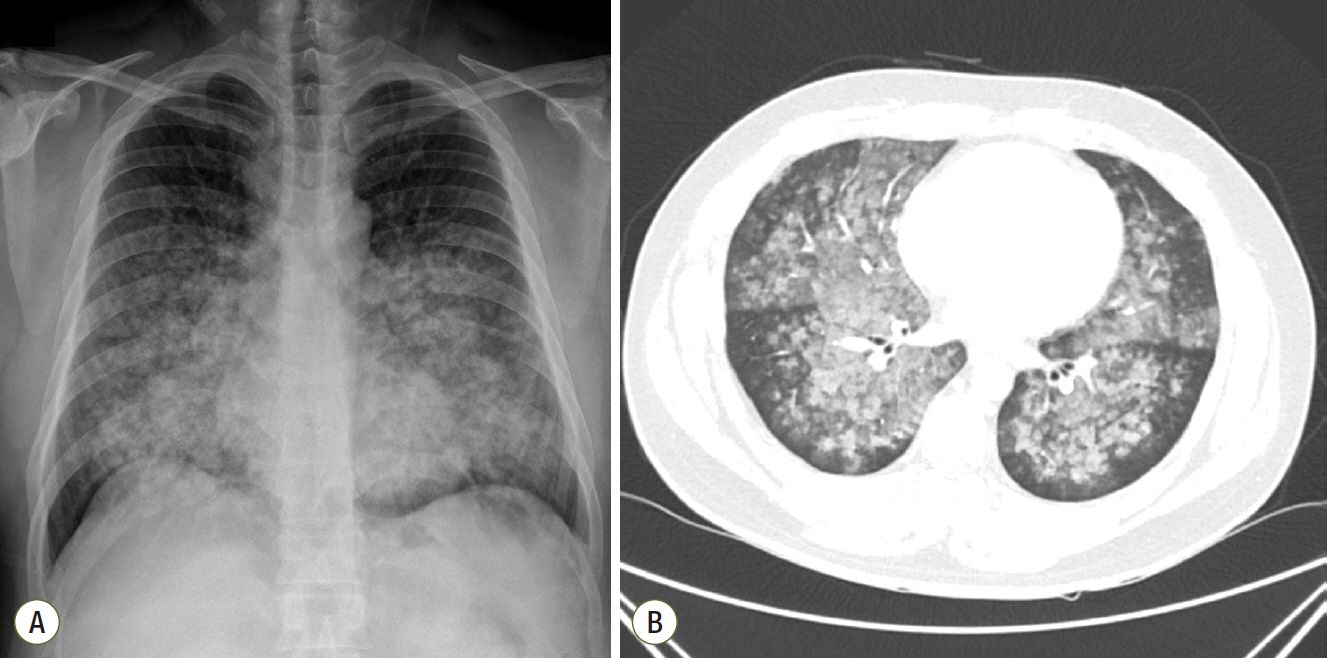
Fig. 1. Initial chest radiographic findings. (A) Initial chest radiograph of the patient showing diffuse bilateral infiltration. (B) Chest computed tomography showing diffuse ground glass opacities and consolidation with centrilobular pattern involving both lungs suggesting diffuse alveolar hemorrhage or acute hypersensitivity pneumonitis.
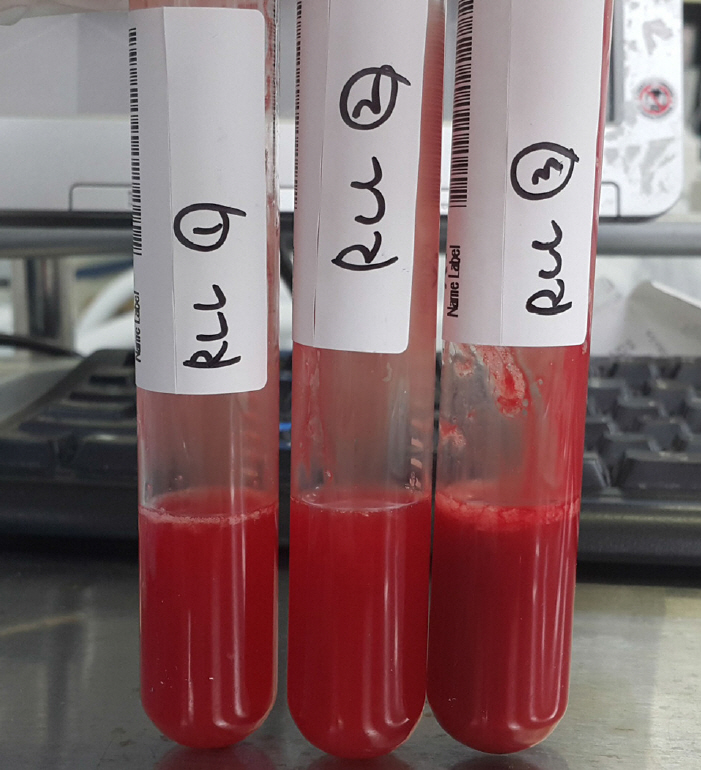
Fig. 2. Result of bronchoalveolar lavage. Bronchoalveolar lavage showing typical progressively bloody returns in the sequential aliquots.
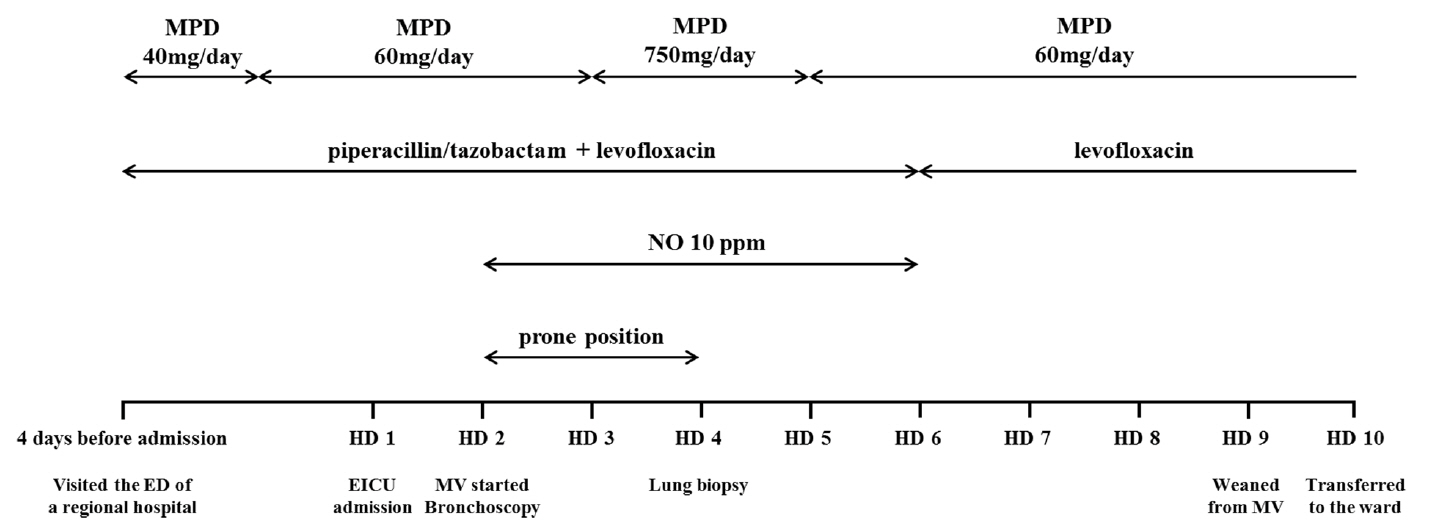
Fig. 3. Summary of key events and the treatment. MPD: methylprednisolone; NO: nitrous oxide; HD: hospital day; ED: emergency department; EICU: emergency intensive care unit; MV: mechanical ventilation.
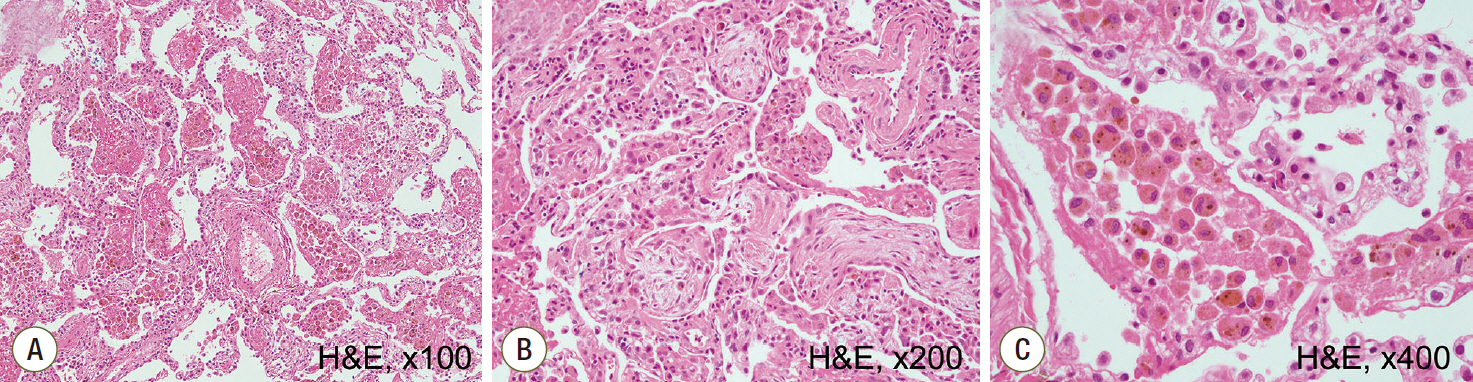
Fig. 4. Histopatholgic findings of open lung biopsy. (A) Diffuse accumulation of red blood cells in the alveolar spaces and interstitial thickening are observed, consistent with diffuse alveolar hemorrhage and organization (hematoxylin and eosin staining (H&E), x100). (B) Some fibroblastic foci are noted in the specimen (H&E, x200). (C) Numerous hemosiderin-laden macrophages and hyperplasia of type II pneumocytes are observed, representing alveolar hemorrhage (H&E, ×400).
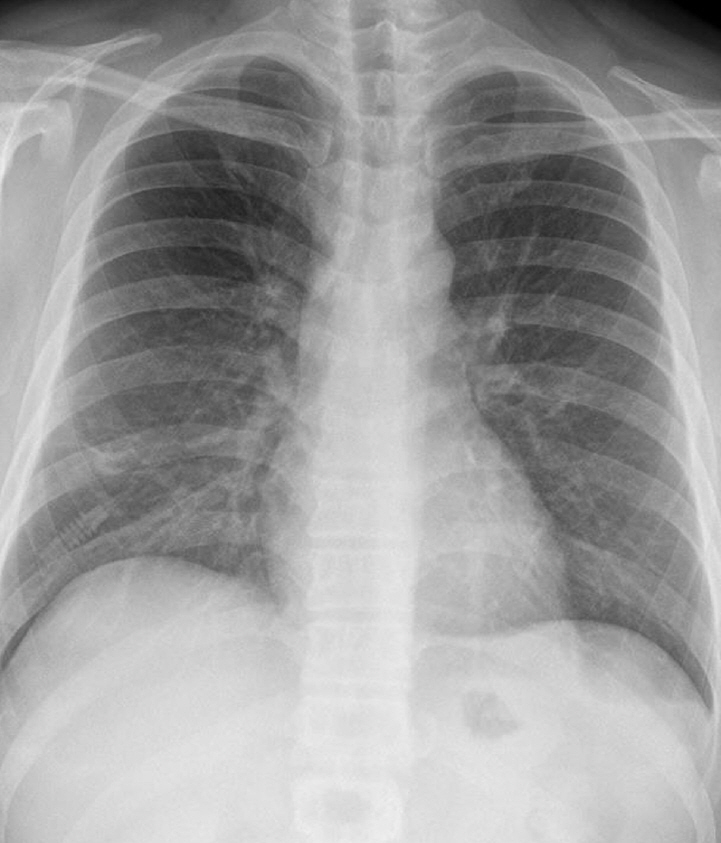
Fig. 5. Improved chest radiographic findings after steroid treatment. Chest radiograph of the patient taken on the day of discharge showing that the previously noted bilateral infiltrations have resolved.
Reference
-
References
1. Lara AR, Schwarz MI. Diffuse alveolar hemorrhage. Chest. 2010; 137:1164–71.
Article2. Selman M, Pardo A, King TE Jr. Hypersensitivity pneumonitis: insights in diagnosis and pathobiology. Am J Respir Crit Care Med. 2012; 186:314–24.3. Seifert SA, Von Essen S, Jacobitz K, Crouch R, Lintner CP. Organic dust toxic syndrome: a review. J Toxicol Clin Toxicol. 2003; 41:185–93.
Article4. Suzuki Y, Imokawa S, Nihashi F, Uto T, Sato J, Suda T. Diffuse alveolar hemorrhage caused by exposure to organic dust. Respir Med Case Rep. 2015; 15:59–61.
Article5. Blanc PD. Husker days and fever nights: counting cases of organic dust toxic syndrome. Chest. 1999; 116:1157–8.6. Christiani DC. Organic dust toxic syndrome. Preventing occupational disease and injury. 2nd ed. In : Levy BS, Wagner GR, Rest KM, Weeks JK, editors. Washington, DC: American Public Health Association;2005. –368.7. Saeed MM, Woo MS, MacLaughlin EF, Margetis MF, Keens TG. Prognosis in pediatric idiopathic pulmonary hemosiderosis. Chest. 1999; 116:721–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute respiratory failure due to diffuse alveolar hemorrhage in mycoplasma pneumonia
- Factors Affecting the Use of Medical Services by Workers with Respiratory Diseases
- Association Between Organic Dust Exposure and Adult-Asthma: A Systematic Review and Meta-Analysis of Case-Control Studies
- Acute Respiratory Distress Syndrome With Alveolar Hemorrhage due to Strongyloidiasis Hyperinfection in an Older Patient
- Association between Perceived Susceptibility to Fine Dust Exposure and Wearing Masks, Attitude toward Respiratory Disease Prevention Education in Farmers
