A Case of Capecitabine-Induced Sarcoidosis
- Affiliations
-
- 1Center for Lung Cancer, National Cancer Center, Goyang, Korea. jekyde7@gmail.com
- 2Department of Pulmonary and Critical Care Medicine, Gachon University Gil Hospital, Incheon, Korea.
- 3Center for Colorectal Cancer, National Cancer Center, Goyang, Korea.
Abstract
- Sarcoidosis is an inflammatory disease involving multiple-organs with an unknown cause. The new onset of sarcoidosis associated with therapeutic agents has been observed in 3 clinical settings; tumor necrosis factor antagonists in autoimmune rheumatologic diseases, interferon alpha with or without ribavirin in patients with chronic hepatitis C or melanoma, and antineoplastic agent-associated sarcoidosis in patients with hematologic malignancies. Here, we report a female patient who developed sarcoidosis after capecitabine treatment as an adjuvant chemotherapy for sigmoid colon cancer. To our knowledge, this is the first report of a capecitabine-induced sarcoidosis.
Keyword
MeSH Terms
Figure
-

Figure 1 Chest radiography prior to capecitabine chemotherapy (A) shows no abnormality. After chemotherapy (B), bilateral hilar adenopathies and parenchymal infiltrates in the left upper lung field are observed. Three months after the discontinuation of capecitabine (C), bilateral hilar adenopathies and parenchymal infiltrates are not observed.

Figure 2 There are no unusual findings in the lungs and mediastinum regarding the chest computed tomography (CT) taken before capecitabine chemotherapy (A, D). After the chemotherapy (B, E), subcarinal and hilar lymph nodes enlargement, beaded bronchovascular bundle, and multiple scattered tiny nodules are observed on the chest CT. Three months after the discontinuation of capecitabine (C, F), the CT shows no subcarinal or hilar lymph node enlargement, and a decrease in size and the number of tiny nodules compared with previous CT images.
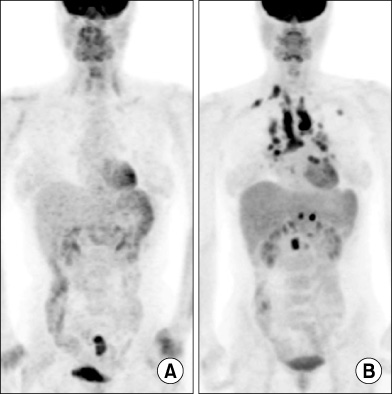
Figure 3 There is no abnormal hypermetabolic lesion except in the sigmoid colon before capecitabine chemotherapy on positiron emission tomography-computed tomography scan (A). After the chemotherapy (B), multiple hypermetabolic lesions suggesting lymphadenopathies are observed in right supraclavicular, mediastinal, hilar, and retroperitoneal areas. A hypermetabolic lesion is also observed in the left upper lung field.
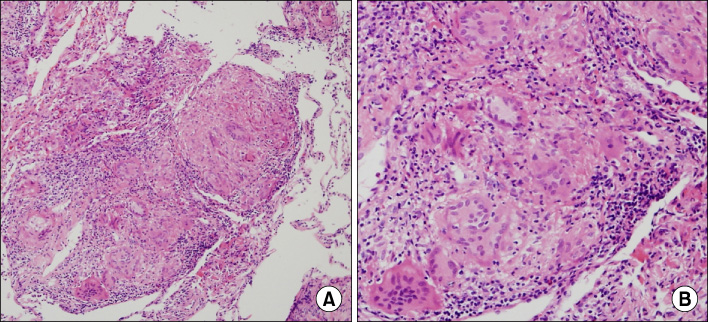
Figure 4 Microscopic finding of transbronchial lung biopsy specimens show multiple noncaseating granulomas (H&E stain; A, ×100; B, ×200).
Reference
-
1. Baughman RP, Culver DA, Judson MA. A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med. 2011. 183:573–581.2. Morgenthau AS, Iannuzzi MC. Recent advances in sarcoidosis. Chest. 2011. 139:174–182.3. Newman LS, Rose CS, Bresnitz EA, Rossman MD, Barnard J, Frederick M, et al. A case control etiologic study of sarcoidosis: environmental and occupational risk factors. Am J Respir Crit Care Med. 2004. 170:1324–1330.4. Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H Jr, Bresnitz EA, et al. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001. 164(10 Pt 1):1885–1889.5. Mikhail SE, Sun JF, Marshall JL. Safety of capecitabine: a review. Expert Opin Drug Saf. 2010. 9:831–841.6. Clementine RR, Lyman J, Zakem J, Mallepalli J, Lindsey S, Quinet R. Tumor necrosis factor-alpha antagonist-induced sarcoidosis. J Clin Rheumatol. 2010. 16:274–279.7. Ramos-Casals M, Perez-Alvarez R, Perez-de-Lis M, Xaubet A, Bosch X. BIOGEAS Study Group. Pulmonary disorders induced by monoclonal antibodies in patients with rheumatologic autoimmune diseases. Am J Med. 2011. 124:386–394.8. Ramos-Casals M, Mañá J, Nardi N, Brito-Zerón P, Xaubet A, Sánchez-Tapias JM, et al. Sarcoidosis in patients with chronic hepatitis C virus infection: analysis of 68 cases. Medicine (Baltimore). 2005. 84:69–80.9. Gayet AR, Plaisance P, Bergmann JF, Mouly S. Development of sarcoidosis following completion of treatment for hepatitis C with pegylated interferon-{alpha2}a and ribavirin: a case report and literature review. Clin Med Res. 2010. 8:163–167.10. Heinzerling LM, Anliker MD, Müller J, Schlaeppi M, von Moos R. Sarcoidosis induced by interferon-alpha in melanoma patients: incidence, clinical manifestations, and management strategies. J Immunother. 2010. 33:834–839.11. López V, Molina I, Monteagudo C, Jordá E. Cutaneous sarcoidosis developing after treatment with pegylated interferon and ribavirin: a new case and review of the literature. Int J Dermatol. 2011. 50:287–291.12. Papanikolaou IC, Sharma OP. The relationship between sarcoidosis and lymphoma. Eur Respir J. 2010. 36:1207–1209.13. Cohen PR, Kurzrock R. Sarcoidosis and malignancy. Clin Dermatol. 2007. 25:326–333.14. Yao M, Funk GF, Goldstein DP, DeYoung BR, Graham MM. Benign lesions in cancer patients: Case 1. Sarcoidosis after chemoradiation for head and neck cancer. J Clin Oncol. 2005. 23:640–641.15. Kim DS. Sarcoidosis in Korea: report of the Second Nationwide Survey. Sarcoidosis Vasc Diffuse Lung Dis. 2001. 18:176–180.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Capecitabine and Cisplatin-induced Cutaneous Hyperpigmentation
- Transient Mutism Related to Capecitabine-Induced Acute Toxic Leukoencephalopathy
- A Case of Coexistent Cutaneous Sarcoidosis in a Patient with Tuberculous Pleurisy
- A Case of Ichthyosiform Sarcoidosis
- Hand-foot Syndrome Due to Capecitabine
