Small-Group Counseling in a Modified Tinnitus Retraining Therapy for Chronic Tinnitus
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, The Catholic University of Korea College of Medicine, Seoul, Korea. sypak@catholic.ac.kr
Abstract
OBJECTIVES
The authors have treated chronic tinnitus patients using a combination of a simplified tinnitus retraining therapy (TRT) and medications, which we called modified TRT. In this clinical setting, we have attempted small-group counseling to find a time-effective equivalent of individual counseling. The aim of the present study was to evaluate the effectiveness of small-group counseling by comparing the treatment outcomes between individual and small-group counseling.
METHODS
The patients who had distressing chronic tinnitus with normal hearing or mild hearing loss were included. The subjects were placed into the small-group (group 1:4) or the individual (group 1:1) counseling group, and underwent a modified TRT composed of a single session of directive counseling and ambient sound stimulation. In addition, alprazolam (0.25 mg) and ginkgo biloba extract (80 mg) were administered orally to the subjects for 3 months. The 3- and 6- month outcomes were assessed using the follow-up rates and tinnitus severity scores: awareness, tinnitus handicap inventory (THI), loudness, annoyance, and effect on life. The treatment responses were classified as improvement, no changes, and worsening.
RESULTS
Of the total 149 patients (77 in group 1:1; 72 in group 1:4), 104 patients completed the protocol at 3 months, and 55 patients at 6 months. The follow-up rates were similar in both groups. Over the period of 6 months, all scores declined significantly except the loudness score at 3 months in both groups. Treatment responses showed no between-group differences. The success rate based on THI was 70% in group 1:1, and 64% in group 1:4 at 6 months.
CONCLUSION
The small-group counseling of our modified TRT was comparable to the individual counseling for tinnitus relief. We suggest that this protocol can be implemented effectively in any crowded otolaryngology clinics.
MeSH Terms
Figure
-
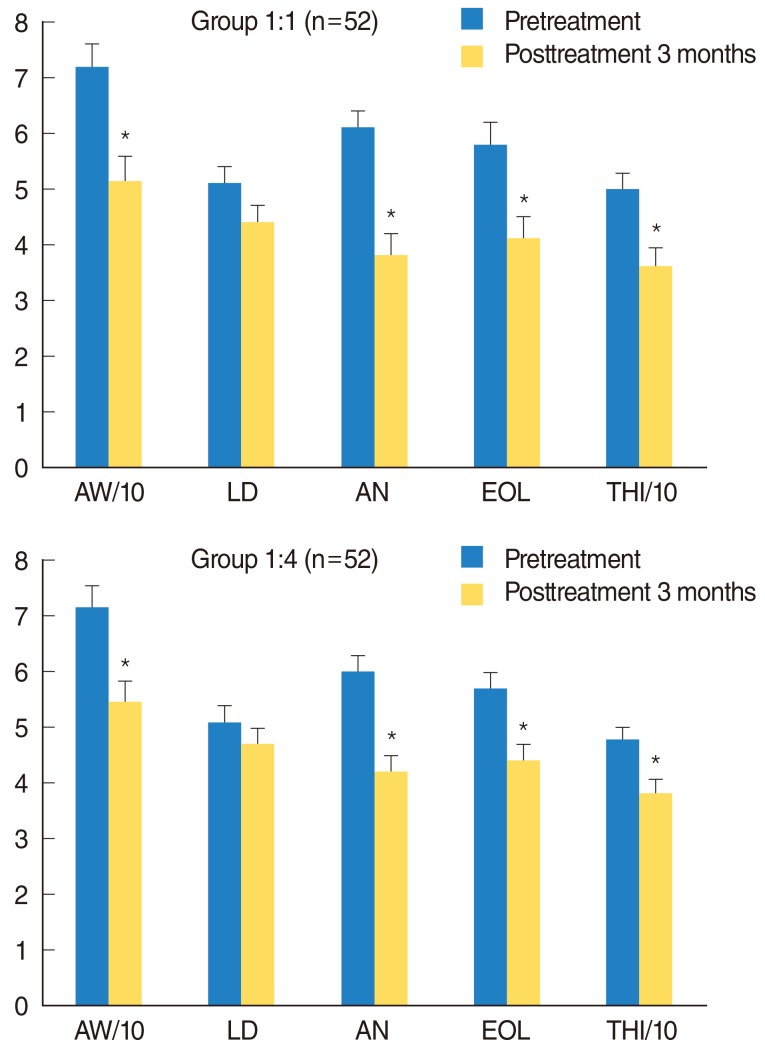
Fig. 1 Changes in tinnitus severity scores at 3 months after modified tinnitus retraining therapy. All scores except LD improved significantly in both groups (*P<0.05 vs. pretreatment scores, paired t-test). AW, awareness; LD, loudness; AN, annoyance; EOL, effect on daily life; THI, tinnitus handicap inventory. Error bars indicate SE.
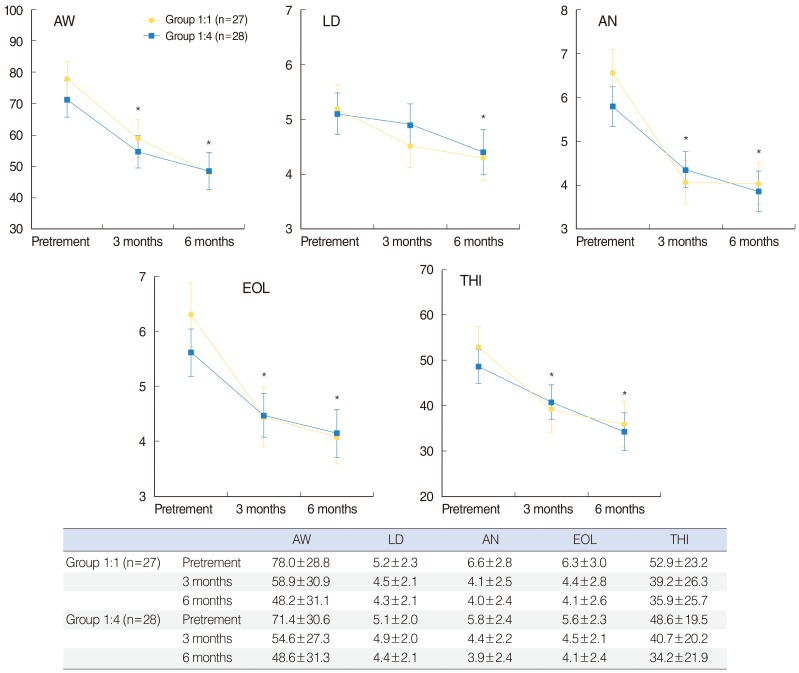
Fig. 2 Changes in tinnitus severity scores at 3- and 6-months after modified tinnitus retraining therapy. The pretreatment scores are not different between the groups (t test). All scores declined significantly throughout 6 months without between-group difference (*P<0.01 vs. pre-Tx scores, repeated-measures ANOVA). The slow declines from the 3- to 6-month values are not statistically significant. Data presented in the table are mean±SD. Error bars indicate SE. AW, awareness; LD, loudness; AN, annoyance; EOL, effect on daily life; THI, tinnitus handicap inventor.
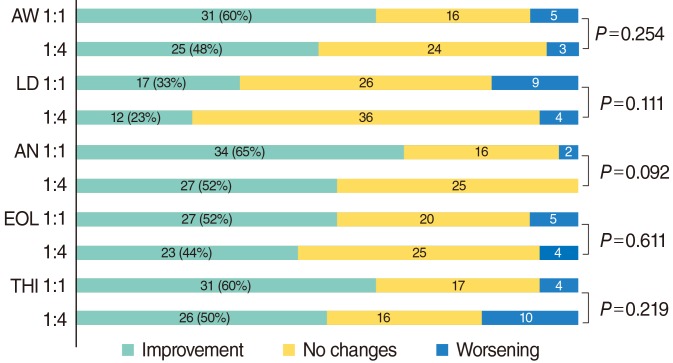
Fig. 3 Therapeutic outcomes based on each tinnitus severity score at the 3-month assessment. Data presented are number of patients. Improvement/worsening=a decrease/an increase of ≥ 20 points in the AW score; ≥ 2 points in each of the LD, AN, and EOL score; ≥ 20% with respect to the initial value in the THI score. 1:1=group 1:1 (n=52); 1:4=group 1:4 (n=52), chi-square test. AW, awareness; LD, loudness; AN, annoyance; EOL, effect on daily life; THI, tinnitus handicap inventor.
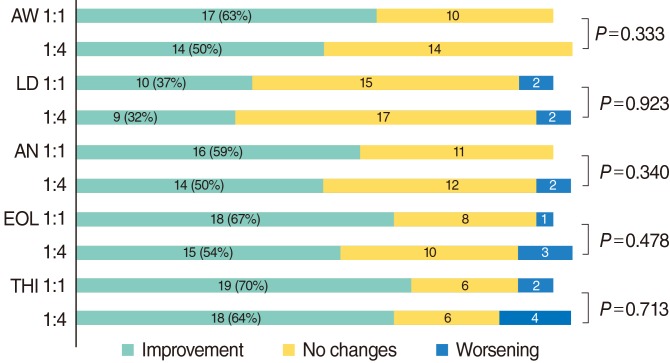
Fig. 4 Therapeutic outcomes based on each tinnitus severity score at the 6-month assessment. 1:1=group 1:1 (n=27); 1:4=group 1:4 (n=28), chi-square test. AW, awareness; LD, loudness; AN, annoyance; EOL, effect on daily life; THI, tinnitus handicap inventor.
Reference
-
1. Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy: a different view on tinnitus. ORL J Otorhinolaryngol Relat Spec. 2006; 3. 68(1):23–29. PMID: 16514259.
Article2. Jastreboff PJ. Tinnitus retraining therapy. Prog Brain Res. 2007; 166:415–423. PMID: 17956806.
Article3. Bauer CA, Brozoski TJ. Assessing tinnitus and prospective tinnitus therapeutics using a psychophysical animal model. J Assoc Res Otolaryngol. 2001; 3. 2(1):54–64. PMID: 11545150.
Article4. Shulman A, Strashun AM, Goldstein BA. GABAA-benzodiazepine-chloride receptor-targeted therapy for tinnitus control: preliminary report. Int Tinnitus J. 2002; Jan-Jun. 8(1):30–36. PMID: 14763233.5. Brozoski TJ, Bauer CA, Caspary DM. Elevated fusiform cell activity in the dorsal cochlear nucleus of chinchillas with psychophysical evidence of tinnitus. J Neurosci. 2002; 3. 22(6):2383–2390. PMID: 11896177.
Article6. Kaltenbach JA, Zhang J, Finlayson P. Tinnitus as a plastic phenomenon and its possible neural underpinnings in the dorsal cochlear nucleus. Hear Res. 2005; 8. 206(Jan-Feb):200–226. PMID: 16081009.
Article7. Kaltenbach JA. The dorsal cochlear nucleus as a contributor to tinnitus: mechanisms underlying the induction of hyperactivity. Prog Brain Res. 2002; Jan-Jun. 166:89–106. PMID: 17956775.
Article8. Auo HJ, Park KH, Yeo SW, Chang KH, Choi HG, Choi BJ, et al. Treatment response of modified tinnitus retraining therapy with medical therapy in the patients with tinnitus. Korean J Otorhinolaryngol-Head Neck Surg. 2009; 8. 52(8):648–654.
Article9. Henry JA, Jastreboff MM, Jastreboff PJ, Schechter MA, Fausti SA. Guide to conducting tinnitus retraining therapy initial and follow-up interviews. J Rehabil Res Dev. 2003; Mar-Apr. 40(2):157–177. PMID: 15077641.
Article10. Newman CW, Jacobson GP, Spitzer JB. Development of the tinnitus handicap inventory. Arch Otolaryngol Head Neck Surg. 1996; 2. 122(2):143–148. PMID: 8630207.
Article11. Kim JH, Lee SY, Kim CH, Lim SL, Shin JN, Chung WH, et al. Reliability and validity of a Korean adaptation of the tinnitus handicap inventory. Korean J Otolaryngol-Head Neck Surg. 2002; 4. 45(4):328–334.12. Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy for patients with tinnitus and decreased sound tolerance. Otolaryngol Clin North Am. 2003; 4. 36(2):321–336. PMID: 12856300.
Article13. Johnson RM, Brummett R, Schleuning A. Use of alprazolam for relief of tinnitus: a double-blind study. Arch Otolaryngol Head Neck Surg. 1993; 8. 119(8):842–845. PMID: 8343245.
Article14. Jalali MM, Kousha A, Naghavi SE, Soleimani R, Banan R. The effects of alprazolam on tinnitus: a cross-over randomized clinical trial. Med Sci Monit. 2009; 11. 15(11):PI55–PI60. PMID: 19865063.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effectiveness of the Directive Counseling in Tinnitus Retraining Therapy
- Tinnitus Retraining Therapy
- Non-pharmacological therapy for tinnitus
- Treatment Response of Modified Tinnitus Retraining Therapy with Medical Therapy in the Patients with Tinnitus
- Clinical Implication and Therapeutic Efficacy of Tinnitus Retraining Therapy
