Tinnitus Retraining Therapy
- Affiliations
-
- 1Soree Ear Clinic, Seoul, Korea. earclinic@hanmail.net
- KMID: 2164670
- DOI: http://doi.org/10.7599/hmr.2016.36.2.120
Abstract
- According to the Jastreboff's neurophysiological model of tinnitus, if negative associations are attached to the tinnitus signal, tinnitus is perceived to be a threat or a danger and it activates the autonomic nervous and limbic systems. Consequently patient's awareness of tinnitus is heightened and so patient perceives it to be louder and more persistent. Jastreboff and Hazell started tinnitus retraining therapy (TRT) based on the neurophysiological model of tinnitus. The purpose of TRT is blocking tinnitus from activating the sympathetic nervous and limbic systems (habituation of reaction) and from reaching the cerebral cortex (habituation of perception). TRT is composed of two components directive counseling that tries to reclassify tinnitus into the meaningless stimuli and sound therapy that decreases the relative strength of the tinnitus signal. Physicians try to put patient's tinnitus into the territory of meaningless stimuli through retraining the brain (habituation of reaction). Because the brain habituates all unimportant stimuli, if habituation of reaction is fully achieved, habituation of perception will follow automatically. In most clinical results, clinical success rates of TRT approach or exceed 80% improvement. Early improvement can be achieved during the first few months, followed by additional progressive improvement. It should be recommended that the patient continue treatment at least 18 months.
Keyword
Figure
-

Fig. 1 The Jastreboff's neurophysiological model of tinnitus. Initially, the tinnitus related neuronal activity is generated at the peripheral auditory system. The subconscious level of the brain may detect this signal. After then, the auditory cortical levels perceive and evaluate this signal. Tinnitus is evaluated and compared with information stored in memory. If the person's tinnitus does not have negative associations, tinnitus signal is subsequently interrupted from contacting conscious perception. But, if tinnitus gets some negative associations, it is classified in the category of unpleasant or dangerous stimuli and consequently activates the autonomic nervous and limbic systems, so results in anxiety, stress, panic attacks and loss of wellbeing. This in turn enhances detection of tinnitus, and further enhances the activation of autonomic nervous and limbic systems.

Fig. 2 Ultimate goal of TRT is to retrain the brain to be habituated to tinnitus. Habituation of reaction is preventing tinnitus from activating the sympathetic nervous and limbic systems. If habituation of reaction is fully achieved, patients do not experience negative reactions and habituation of perception will follow automatically, because the brain habituates all unimportant stimuli. If habituation of perception is achieved, tinnitus is blocked before it reaches the consciousness level, and patients do not hear tinnitus. HP, habituation of perception; HLR, habituation of limbic reaction; HAR, habituation of autonomic reaction.
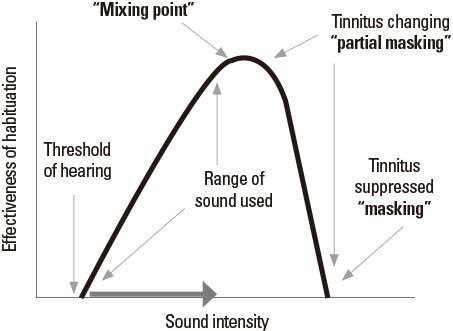
Fig. 3 The relationship between sound generator volume and the effectiveness of habituation. When the sound generator is used, we usually adjust sound generator volume close to the mixing point, in category 1 patients. Mixing point is the volume of sound generator at which the noise just starts to mix with the tinnitus. The effectiveness of habituation increases as volume proceeds to the mixing point. But, after the sound generator volume is louder than mixing point, masking begins and efficacy quickly decreases. Tinnitus should never be masked in TRT, because patients cannot be habituated to tinnitus that they cannot hear.
Cited by 1 articles
-
Tinnitus: Overview
Chul Won Park
Hanyang Med Rev. 2016;36(2):79-80. doi: 10.7599/hmr.2016.36.2.79.
Reference
-
1. Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res. 1990; 8:221–254.
Article2. Jastreboff PJ, Hazell JWP. A neurophysiological approach to tinnitus: clinical implications. Br J Audiol. 1993; 27:7–17.
Article3. Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol. 1996; 17:236–240.4. Davis A, El Refaie A. Tinnitus Handbook. In : Tyler RS, editor. San Diego: Singular Thomson Learning;2000. p. 1–23.5. Jastreboff PJ, Hazell JWP, Graham RL. Neurophysiological model of tinnitus: dependence of the minimal masking level on treatment outcome. Hear Res. 1994; 80:216–232.
Article6. Henry JA, Jastreboff MM, Jastreboff PJ, schechter MA, Fausti SA. Assessment of patients for treatment with tinnitus retraining therapy. J Am Acad Audiol. 2002; 13:523–544.
Article7. Lockwood AH, Salvi RJ, Coad ML, Towsley ML, Wack DS, Murphy BW. The functional neuroanatomy of tinnitus: evidence for limbic system links and neural plasticity. Neurology. 1998; 50:114–120.8. Lockwood AH, Salvi RJ, Burkard RF. Tinnitus. N Engl J Med. 2002; 347:904–910.
Article9. Mirz F, Pedersen B, Ishizu K, Johannsen P, Ovesen T, Stødkilde-Jørgensen H, et al. Positron emission tomography of cortical centers of tinnitus. Hear Res. 1999; 134:133–144.
Article10. Mirz F, Gjedde A, Ishizu K, Pedersen CB. Cortical networks subserving the perception of tinnitus-a PET study. Acta Otolaryngol Suppl. 2000; 543:241–243.11. Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1996; 122:143–148.
Article12. Newman CW, Sandridge SA, Jacobson GP. Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. J Am Acad Audiol. 1998; 9:153–160.13. Adamchic I, Langguth B, Hauptmann C, Tass PA. Psychometric evaluation of visual analog scale for the assessment of chronic tinnitus. Am J Audiol. 2012; 21:215–225.
Article14. Lee HK, Kim CW, Chung MH, Kim HN. The effectiveness of the directive counseling in tinnitus retraining therapy. Korean J Otolaryngol. 2004; 47:217–221.15. Jastreboff PJ. 25 years of tinnitus retraining therapy. HNO. 2015; 63:307–311.
Article16. Lee HK. Tinnitus retraining therapy. Korean J Audiol. 2002; 6:71–75.17. Park SN, Yeo SW, Chung SH, Lee SJ, Park YS, Suh BD. Clinical implication and therapeutic efficacy of tinnitus retraining therapy. Korean J Otolaryngol. 2002; 45:231–237.18. Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy (TRT) as a method for treatment of tinnitus and hyperacusis patients. J Am Acad Audiol. 2000; 11:162–177.19. Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy for patients with tinnitus and decreased sound tolerance. Otolaryngol Clin North Am. 2003; 36:321–336.
Article20. Cima RF, Maes IH, Joore MA, Scheyen DJ, El Refaie A, Baquley DM, et al. Specialised treatment based on cognitive behaviour therapy versus usual care for tinnitus: a randomised controlled trial. Lancet. 2012; 379:1951–1959.
Article21. Phillips JS, McFerran D. Tinnitus Retraining Therapy (TRT) for tinnitus. Cochrane Database Syst Rev. 2010; 17(3):CD007330.
Article22. Henry JA, Schechter MA, Zaugg TL, Griest S, Jastreboff PJ, Vernon JA, et al. Outcomes of clinical trial: tinnitus masking versus tinnitus retraining therapy. J Am Acad Audidol. 2006; 17:104–132.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effectiveness of the Directive Counseling in Tinnitus Retraining Therapy
- Clinical Implication and Therapeutic Efficacy of Tinnitus Retraining Therapy
- Psychological Analysis with Symptom Check List-90-Revision in Patients with Tinnitus
- Short Term Effect of Mixed Tinnitus Retraining Therapy
- Non-pharmacological therapy for tinnitus
