Allergy Asthma Immunol Res.
2013 May;5(3):155-161. 10.4168/aair.2013.5.3.155.
Relationships Between Exhaled Nitric Oxide and Atopy Profiles in Children With Asthma
- Affiliations
-
- 1Department of Pediatrics, Hanil General Hospital, Seoul, Korea.
- 2Department of Pediatrics, College of Medicine, Korea University, Seoul, Korea. yoolina@korea.ac.kr
- 3Environmental Health Center for Childhood Asthma, Korea University Anam Hospital, Seoul, Korea.
- 4Department of Pediatrics, Mokpo Hansarang Hospital, Mokpo, Korea.
- 5Allergy Immunology Center, Korea University, Seoul, Korea.
- KMID: 2260335
- DOI: http://doi.org/10.4168/aair.2013.5.3.155
Abstract
- PURPOSE
We examined whether fractional exhaled nitric oxide (FeNO) levels are associated with atopy profiles in terms of mono-sensitization and poly-sensitization in asthmatic children.
METHODS
A total of 119 children underwent an assessment that included FeNO measurements, spirometry, methacholine challenge, and measurement of blood eosinophil count, serum total IgE, and serum eosinophil cationic protein (ECP). We also examined sensitization to five classes of aeroallergens (house dust mites, animal danders, pollens, molds, and cockroach) using skin prick testing. The children were divided into three groups according to their sensitization profiles to these aeroallergens (non-sensitized, mono-sensitized, and poly-sensitized).
RESULTS
The geometric means (range of 1 SD) of FeNO were significantly different between the three groups (non-sensitized, 18.6 ppb [10.0-34.7 ppb]; mono-sensitized, 28.8 ppb [16.6-50.1 ppb]; and poly-sensitized, 44.7 ppb [24.5-81.3 ppb], P=0.001). FeNO levels were correlated with serum total IgE concentrations, peripheral blood eosinophilia, and serum ECP levels to different degrees.
CONCLUSIONS
FeNO levels vary according to the profile of atopy, as determined by positive skin prick test results to various classes of aeroallergens. FeNO is also moderately correlated with serum total IgE, blood eosinophilia, and serum ECP. These results suggest that poly-sensitized asthmatic children may have the highest risk of airway inflammation.
Keyword
MeSH Terms
Figure
-
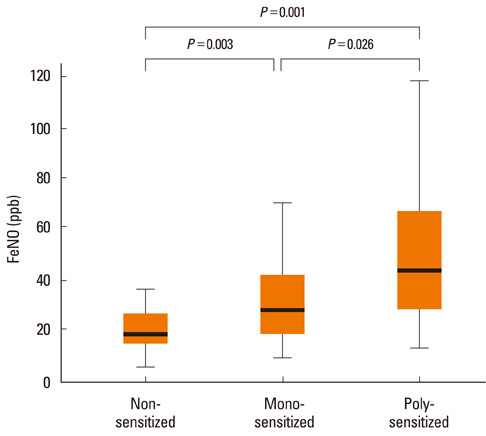
Figure Mean and percentile (10th, 25th, 75th, and 90th) distributions of FeNO in non-sensitized, mono-sensitized, and poly-sensitized asthma groups.
Cited by 1 articles
-
Comparison between exhaled nitric oxide and bronchial challenge with methacholine or adenosine-5'-monophosphate in the diagnosis of childhood asthma
Jisun Yoon, Jun-Sung Park, Hyun-Ju Cho, Eun Lee, Song-I Yang, Soo-Jong Hong, Jinho Yu
Allergy Asthma Respir Dis. 2016;4(2):100-106. doi: 10.4168/aard.2016.4.2.100.
Reference
-
1. Høst A, Halken S. The role of allergy in childhood asthma. Allergy. 2000. 55:600–608.2. Silvestri M, Oddera S, Rossi GA, Crimi P. Sensitization to airborne allergens in children with respiratory symptoms. Ann Allergy Asthma Immunol. 1996. 76:239–244.3. Linn WS, Rappaport EB, Berhane KT, Bastain TM, Avol EL, Gilliland FD. Exhaled nitric oxide in a population-based study of Southern California schoolchildren. Respir Res. 2009. 10:28.4. Thomas PS, Gibson PG, Wang H, Shah S, Henry RL. The relationship of exhaled nitric oxide to airway inflammation and responsiveness in children. J Asthma. 2005. 42:291–295.5. Warke TJ, Fitch PS, Brown V, Taylor R, Lyons JD, Ennis M, Shields MD. Exhaled nitric oxide correlates with airway eosinophils in childhood asthma. Thorax. 2002. 57:383–387.6. Cordeiro D, Rudolphus A, Snoey E, Braunstahl GJ. Utility of nitric oxide for the diagnosis of asthma in an allergy clinic population. Allergy Asthma Proc. 2011. 32:119–126.7. Banovcin P, Jesenak M, Michnova Z, Babusikova E, Nosal S, Mikler J, Fabry J, Barreto M. Factors attributable to the level of exhaled nitric oxide in asthmatic children. Eur J Med Res. 2009. 14:Suppl 4. 9–13.8. Prasad A, Langford B, Stradling JR, Ho LP. Exhaled nitric oxide as a screening tool for asthma in school children. Respir Med. 2006. 100:167–173.9. Hervás D, Milán JM, Garde J. Differences in exhaled nitric oxide in atopic children. Allergol Immunopathol (Madr). 2008. 36:331–335.10. Fitzpatrick AM, Gaston BM, Erzurum SC, Teague WG. National Institutes of Health/National Heart, Lung, and Blood Institute Severe Asthma Research Program. Features of severe asthma in school-age children: atopy and increased exhaled nitric oxide. J Allergy Clin Immunol. 2006. 118:1218–1225.11. National Asthma Education and Prevention Program. National Institutes of Health publication 97-4051. Guidelines for the diagnosis and management of asthma: expert panel report 2. 1997. Bethesda, MD: US Department of Health and Human Services.12. American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995. 152:1107–1136.13. Chai H, Farr RS, Froehlich LA, Mathison DA, McLean JA, Rosenthal RR, Sheffer AL, Spector SL, Townley RG. Standardization of bronchial inhalation challenge procedures. J Allergy Clin Immunol. 1975. 56:323–327.14. American Thoracic Society. European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005. 171:912–930.15. Høst A, Andrae S, Charkin S, Diaz-Vázquez C, Dreborg S, Eigenmann PA, Friedrichs F, Grinsted P, Lack G, Meylan G, Miglioranzi P, Muraro A, Nieto A, Niggemann B, Pascual C, Pouech MG, Rancé F, Rietschel E, Wickman M. Allergy testing in children: why, who, when and how? Allergy. 2003. 58:559–569.16. Storm van's Gravesande K, Moseler M, Kuehr J. The most common phenotypes of sensitization to inhalant allergens in childhood. Clin Exp Allergy. 1997. 27:646–652.17. Yoo Y, Yu J, Kim DK, Choi SH, Koh YY. Coincidence of atopy and its profile (monosensitization/polysensitization) between sibling pairs. Ann Allergy Asthma Immunol. 2005. 95:433–437.18. Piacentini GL, Bodini A, Costella S, Suzuki Y, Zerman L, Peterson CG, Boner AL. Exhaled nitric oxide, serum ECP and airway responsiveness in mild asthmatic children. Eur Respir J. 2000. 15:839–843.19. Malmberg LP, Petäys T, Haahtela T, Laatikainen T, Jousilahti P, Vartiainen E, Mäkelä MJ. Exhaled nitric oxide in healthy nonatopic school-age children: determinants and height-adjusted reference values. Pediatr Pulmonol. 2006. 41:635–642.20. Strunk RC, Szefler SJ, Phillips BR, Zeiger RS, Chinchilli VM, Larsen G, Hodgdon K, Morgan W, Sorkness CA, Lemanske RF Jr. Childhood Asthma Research and Education Network of the National Heart, Lung, and Blood Institute. Relationship of exhaled nitric oxide to clinical and inflammatory markers of persistent asthma in children. J Allergy Clin Immunol. 2003. 112:883–892.21. Moore WC, Bleecker ER, Curran-Everett D, Erzurum SC, Ameredes BT, Bacharier L, Calhoun WJ, Castro M, Chung KF, Clark MP, Dweik RA, Fitzpatrick AM, Gaston B, Hew M, Hussain I, Jarjour NN, Israel E, Levy BD, Murphy JR, Peters SP, Teague WG, Meyers DA, Busse WW, Wenzel SE. National Heart, Lung, Blood Institute's Severe Asthma Research Program. Characterization of the severe asthma phenotype by the National Heart, Lung, and Blood Institute's Severe Asthma Research Program. J Allergy Clin Immunol. 2007. 119:405–413.22. Koh YI, Choi IS, Lim H. Atopy may be related to exercise-induced bronchospasm in asthma. Clin Exp Allergy. 2002. 32:532–536.23. Silvestri M, Sabatini F, Spallarossa D, Fregonese L, Battistini E, Biraghi MG, Rossi GA. Exhaled nitric oxide levels in non-allergic and allergic mono- or polysensitised children with asthma. Thorax. 2001. 56:857–862.24. Kharitonov SA, Barnes PJ. Exhaled markers of pulmonary disease. Am J Respir Crit Care Med. 2001. 163:1693–1722.25. Marshall HE, Stamler JS. NO waiting to exhale in asthma. Am J Respir Crit Care Med. 2000. 161:685–687.26. Bommarito L, Migliore E, Bugiani M, Heffler E, Guida G, Bucca C, de Marco R, Rolla G. ECRHS Turin, Italy Study Group. Exhaled nitric oxide in a population sample of adults. Respiration. 2008. 75:386–392.27. Franklin PJ, Taplin R, Stick SM. A community study of exhaled nitric oxide in healthy children. Am J Respir Crit Care Med. 1999. 159:69–73.28. Duff AL, Platts-Mills TA. Allergens and asthma. Pediatr Clin North Am. 1992. 39:1277–1291.29. van den Toorn LM, Prins JB, de Jongste JC, Leman K, Mulder PG, Hoogsteden HC, Overbeek SE. Benefit from anti-inflammatory treatment during clinical remission of atopic asthma. Respir Med. 2005. 99:779–787.30. Malmberg LP, Turpeinen H, Rytilä P, Sarna S, Haahtela T. Determinants of increased exhaled nitric oxide in patients with suspected asthma. Allergy. 2005. 60:464–468.31. Joseph-Bowen J, de Klerk N, Holt PG, Sly PD. Relationship of asthma, atopy, and bronchial responsiveness to serum eosinophil cationic proteins in early childhood. J Allergy Clin Immunol. 2004. 114:1040–1045.32. Chiron R, Vachier I, Khanbabaee G, Molinari N, Varrin M, Godard P, Chanez P. Impact of rhinitis on asthma control in children: association with FeNO. J Asthma. 2010. 47:604–608.33. Franklin PJ, Stick SM, Le Souëf PN, Ayres JG, Turner SW. Measuring exhaled nitric oxide levels in adults: the importance of atopy and airway responsiveness. Chest. 2004. 126:1540–1545.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Utility of Fractional Exhaled Nitric Oxide in the Diagnosis of Asthma and the Assessment of Asthma Control
- Measurements of fractional exhaled nitric oxide in pediatric asthma
- Clinical Significance of Exhaled Nitric Oxide Concentration in Childhood Asthma
- Exhaled Nitric Oxide Measurement for Asthma Management
- Clinical application of fractional exhaled nitric oxide in pediatric allergic rhinitis
