Multiple Cerebral Infarctions due to Unilateral Traumatic Vertebral Artery Dissection after Cervical Fractures
- Affiliations
-
- 1Department of Neurosurgery, Kyungpook National University Hospital, Daegu, Korea. nsdoctor@naver.com
- KMID: 2163013
- DOI: http://doi.org/10.13004/kjnt.2016.12.1.34
Abstract
- We report a case of multiple symptomatic cerebral infarctions from a traumatic vertebral artery dissection (VAD) after cervical fractures. A 73-year-old man was admitted with stuporous mentality and left hemiparesis after a motor-vehicle accident. A brain computed tomography (CT) scan at admission showed a traumatic subarachnoid hemorrhage on the left parietal lobe. A cervical CT scan showed left lateral mass fractures on C2, C5, and C6, involving the transverse foramen. Cervical spine magnetic resonance imaging (MRI) revealed loss of signal void on the left vertebral artery. Neck CT angiography showed left VAD starting at the C5 level. Brain MRI revealed acute, multiple cerebral infarctions involving the pons, midbrain, thalamus, corpus callosum, and parietal and frontal lobes on diffusion weighted images. The patient was treated conservatively at the intensive care unit in the acute stage to prevent extent of stroke. Aspirin was started for antiplatelet therapy in the chronic stage. The possibility of symptomatic cerebral infarctions due to traumatic VAD following cervical fracture should be considered.
MeSH Terms
-
Aged
Angiography
Aspirin
Brain
Cerebral Infarction*
Cervical Vertebrae
Corpus Callosum
Diffusion
Female
Frontal Lobe
Humans
Intensive Care Units
Magnetic Resonance Imaging
Mesencephalon
Neck
Paresis
Parietal Lobe
Pons
Rabeprazole
Spinal Fractures
Spine
Stroke
Stupor
Subarachnoid Hemorrhage, Traumatic
Thalamus
Tomography, X-Ray Computed
Vertebral Artery
Vertebral Artery Dissection*
Aspirin
Figure
-
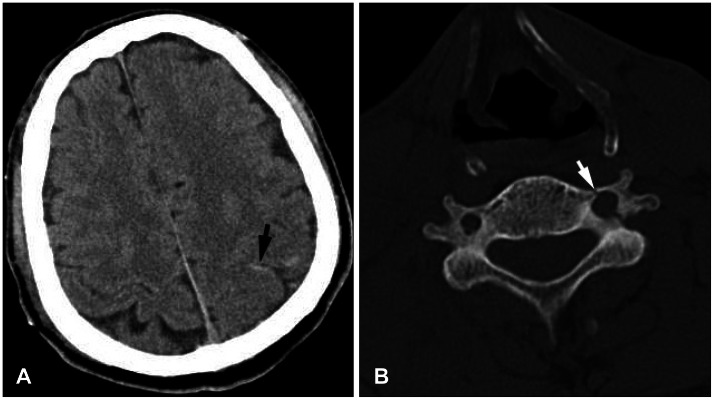
FIGURE 1 A: Brain computed tomography (CT) scan showing traumatic subarachnoid hemorrhage (arrow) on the left parietal lobe after trauma. B: Cervical CT scan demonstrating fracture of the left transverse process of C6 (arrow) with encroachment on the neural foramen.
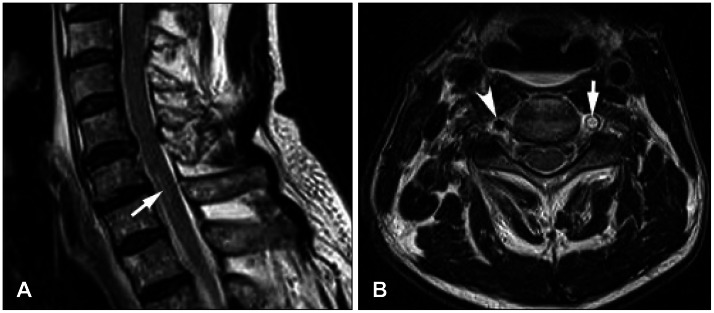
FIGURE 2 Cervical spine magnetic resonance imaging. A: Sagittal T2 weighted image showing a high signal (arrow) on the C6-7 cord on a sagittal image. B: Loss of the signal void was detected on the left vertebral artery (arrow) on the C6 axial T2 weighted image. See the normal signal void of the right vertebral artery (arrowhead).

FIGURE 3 Neck computed tomography angiography showing obliteration of the V2 segment on the left vertebral artery (arrow).
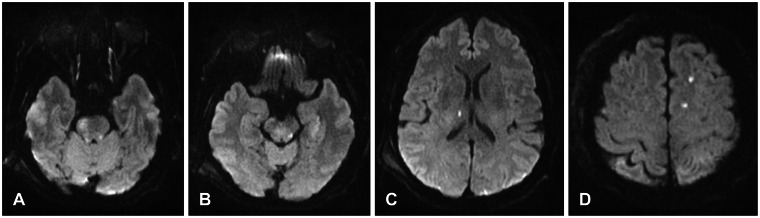
FIGURE 4 Brain magnetic resonance imaging showing multiple high signals on diffusion weighted images of the pons (A), midbrain (B), thalamus (C), and frontal lobe (D).

FIGURE 5 Brain computed tomography scan showing chronic subdural hematomas on both frontal lobes (*) 4 months after the trauma.
Cited by 1 articles
-
A Case of Posterior Inferior Cerebellar Artery Infarction after Cervical Chiropractic Manipulation
Do Kyeun Jeong, Sung-Kyun Hwang
Korean J Neurotrauma. 2018;14(2):159-163. doi: 10.13004/kjnt.2018.14.2.159.
Reference
-
1. Giacobetti FB, Vaccaro AR, Bos-Giacobetti MA, Deeley DM, Albert TJ, Farmer JC, et al. Vertebral artery occlusion associated with cervical spine trauma. A prospective analysis. Spine (Phila Pa 1976). 1997; 22:188–192. PMID: 9122799.2. Hoffmann M, Sacco RL, Chan S, Mohr JP. Noninvasive detection of vertebral artery dissection. Stroke. 1993; 24:815–819. PMID: 8506553.
Article3. Miyachi S, Okamura K, Watanabe M, Inoue N, Nagatani T, Takagi T. Cerebellar stroke due to vertebral artery occlusion after cervical spine trauma. Two case reports. Spine (Phila Pa 1976). 1994; 19:83–88. PMID: 8153813.4. Parent AD, Harkey HL, Touchstone DA, Smith EE, Smith RR. Lateral cervical spine dislocation and vertebral artery injury. Neurosurgery. 1992; 31:501–509. PMID: 1407430.
Article5. Schellinger PD, Schwab S, Krieger D, Fiebach JB, Steiner T, Hund EF, et al. Masking of vertebral artery dissection by severe trauma to the cervical spine. Spine (Phila Pa 1976). 2001; 26:314–319. PMID: 11224870.
Article6. Schwarz N, Buchinger W, Gaudernak T, Russe F, Zechner W. Injuries to the cervical spine causing vertebral artery trauma: case reports. J Trauma. 1991; 31:127–133. PMID: 1986118.7. Suechting RL, French LA. Posterior inferior cerebellar artery syndrome; following a fracture of the cervical vertebra. J Neurosurg. 1955; 12:187–189. PMID: 14368351.8. Tekin S, Aykut-Bingöl C, Aktan S. Case of intracranial vertebral artery dissection in young age. Pediatr Neurol. 1997; 16:67–70. PMID: 9044407.
Article9. Watridge CB, Muhlbauer MS, Lowery RD. Traumatic carotid artery dissection: diagnosis and treatment. J Neurosurg. 1989; 71:854–857. PMID: 2585077.
Article10. Willis BK, Greiner F, Orrison WW, Benzel EC. The incidence of vertebral artery injury after midcervical spine fracture or subluxation. Neurosurgery. 1994; 34:435–441. discussion 441–discussion 442. PMID: 8190218.
Article11. Wirbel R, Pistorius G, Braun C, Eichler A, Mutschler W. Bilateral vertebral artery lesion after dislocating cervical spine trauma. A case report. Spine (Phila Pa 1976). 1996; 21:1375–1379. discussion 1380PMID: 8725932.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Cerebral Infarctions from Vertebral Artery Dissection Induced by Severe Coughing
- Vertebral Artery Dissection Presenting with Acute Infarction in Cervical Spinal Cord and Cerebellum
- Delayed Vertebral Artery Dissection after Posterior Cervical Fusion with Traumatic Cervical Instability: A Case Report
- Reversible Cerebral Vasoconstriction Syndrome with Concurrent Anterior Cerebral Artery Dissection
- Vertebral Artery Dissection Presented with Monoplegia by Cervical Radiculopathy
