Korean J Hematol.
2005 Dec;40(4):266-270. 10.5045/kjh.2005.40.4.266.
Reduced Intensity Conditioning Regimen Followed by Allogeneic Peripheral Blood Stem Cell Transplantation for Acute Panmyelosis with Myelofibrosis
- Affiliations
-
- 1Department of Internal Medicine, Wonkwang University School of Medicien, Iksan, Korea. mrpark21@wonkwang.ac.kr
- 2Department of Laboratory Medicine, Wonkwang University School of Medicien, Iksan, Korea.
- KMID: 2083465
- DOI: http://doi.org/10.5045/kjh.2005.40.4.266
Abstract
- A 44-year-old male presented with a month history of exertional dyspnea and dizziness. A peripheral blood smear revealed a pancytopenia with 3% of blasts. We were not able to obtain a bone marrow aspirate, but a biopsy specimen showed hypercellularity, proliferation of trilineage cell lines (panmyelosis) with extensive myelofibrosis, and clusters of immature cells at the paratrabecular area. After remission induction therapy with idarubicin 12mg/m2 (D1-3) and cytosine arabinoside 100mg/m2 (D1-7), the bone marrow blast count was decreased, but the marrow fibrosis and pancytopenia persisted. Peripheral blood stem cell transplantation from his HLA-matched brother was performed after administering fludarabine 30mg/m2 for 5 days and busulfan 3.2mg/kg for 2 days. Early engraftment occurred and the bone marrow reticulin fibrosis disappeared. Full-donor chimerism was demonstrated at day 22 by performing short tandem repeats analysis and this was maintained for 1 year. The patient has survived 20 months after transplantation without any complication.
Keyword
MeSH Terms
Figure
-
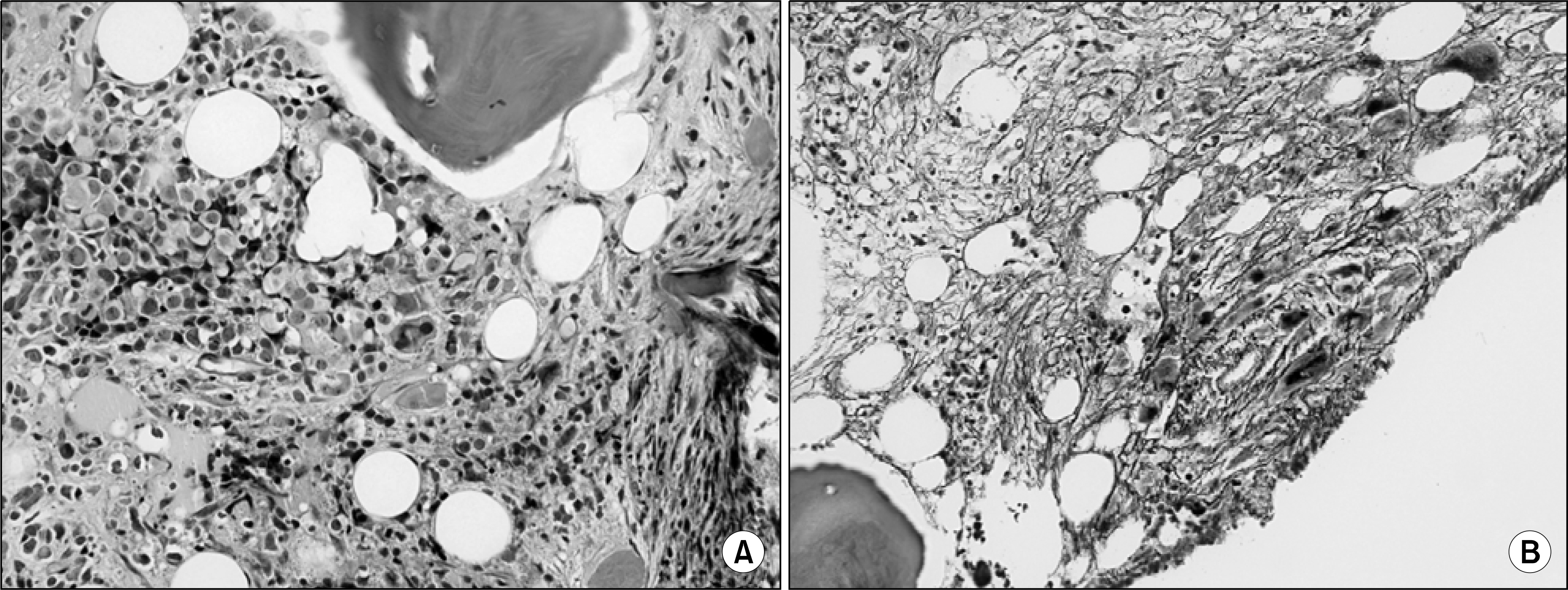
Fig. 1. Bone marrow biopsy section at the time of diagnosis reveals marked fibrosis and some immature cells (A, H&E stain, ×400), and shows extensive reticulin fibrosis (B, reticulin stain, ×400).
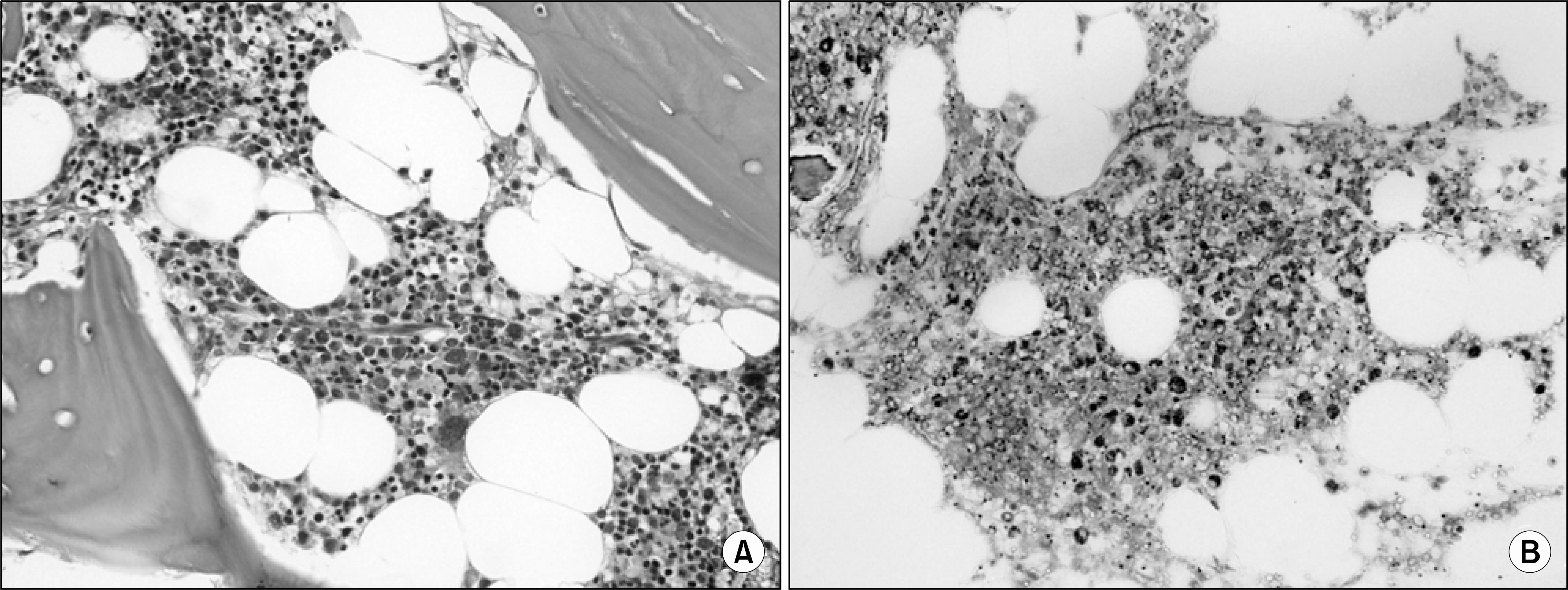
Fig. 2. After 1 year of stem cell transplantation, bone marrow biopsy section shows the normocellularity without myelofibrosis (A, H&E stain, ×400), and no evidence of reticulin fibrosis (B, reticulin stain, ×400).
Reference
-
1). Brunning R, Matutes E, Flandrin G, et al. Acute myeloid leukaemia not otherwise categorised. Jaffe E, Harris N, Stein H, Vardiman J, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 1st ed.Lyon: IARC Press;2006. p. 103–4.2). Thiele J, Kvasnicka HM, Schmitt-Graeff A. Acute panmyelosis with myelofibrosis. Leuk Lymphoma. 2004; 45:681–7.
Article3). Smith JW, Shulman HM, Thomas ED, Fefer A, Buckner CD. Bone marrow transplantation for acute myelosclerosis. Cancer. 1981; 48:2198–203.
Article4). Wolf JL, Spruce WE, Bearman RM, et al. Reversal of acute (“malignant”) myelosclerosis by allogeneic bone marrow transplantation. Blood. 1982; 59:191–3.
Article5). Rozman C, Granena A, Hernandez-Prieto M, Vela E, Brugues R. Bone-marrow transplantation for acute myelofibrosis. Lancet. 1982; 1:618.
Article6). Kroener JF, McMillan R, Beutler E. Acute myelofibrosis. Treatment with allogeneic bone marrow transplantation. JAMA. 1983; 249:1189–90.
Article7). Maruta A, Matsuzaki M, Kanamori H, et al. Allogeneic bone marrow transplantation as primary treatment in acute myelofibrosis. Rinsho Ketsueki. 1989; 30:904–9.8). Lee YJ, Park MR. A case of acute panmyelosis with myelofibrosis. Korean J Lab Med. 2004; 24:207–11.9). Suvajdzic N, Marisavljevic D, Kraguljac N, et al. Acute panmyelosis with myelofibrosis: clinical, immunophenotypic and cytogenetic study of twelve cases. Leuk Lymphoma. 2004; 45:1873–9.
Article10). Cervantes F, Rovira M, Urbano-Ispizua A, Rozman M, Carreras E, Montserrat E. Complete remission of idiopathic myelofibrosis following donor lymphocyte infusion after failure of allogeneic transplantation: demonstration of a graft-versus-myelofibrosis effect. Bone Marrow Transplant. 2000; 26:697–9.
Article11). Byrne JL, Beshti H, Clark D, et al. Induction of remission after donor leucocyte infusion for the treatment of relapsed chronic idiopathic myelofibrosis following allogeneic transplantation: evidence for a ‘graft vs. myelofibrosis’ effect. Br J Haematol. 2000; 108:430–3.
Article12). Hessling J, Kroger N, Werner M, et al. Dose-reduced conditioning regimen followed by allogeneic stem cell transplantation in patients with myelofibrosis with myeloid metaplasia. Br J Haematol. 2002; 119:769–72.
Article13). Devine SM, Hoffman R, Verma A, et al. Allogeneic blood cell transplantation following reduced-intensity conditioning is effective therapy for older patients with myelofibrosis with myeloid metaplasia. Blood. 2002; 99:2255–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reduced-intensity conditioning versus myeloablative conditioning allogeneic stem cell transplantation for patients with myelofibrosis
- A Case of Acute Panmyelosis with Myelofibrosis
- Acute Myeloid Leukemia with Persistent Marrow Aplasia after Chemotherapy Treated with Reduced-Intensity Allogeneic Stem Cell Transplantation
- Allogeneic Stem Cell Transplantation for Patients with Advanced Hematological Malignancies: Comparison of Fludarabine-based Reduced Intensity Conditioning versus Myeloablative Conditioning
- Two Cases of Generalized Vitiligo after Allogeneic Stem Cell Transplantation
