Clinical Benefits and Complications of Cryotherapy in Advanced Lung Cancer with Central Airway Obstruction
- Affiliations
-
- 1Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. pusarang@gmail.com
- 2Guro Hospital, Korea University Medical Center, Seoul, Korea.
- KMID: 1970177
- DOI: http://doi.org/10.4046/trd.2008.64.4.272
Abstract
-
BACKGROUND: The efficacy of the use of the interventional bronchoscope for palliation of patients with central airway obstruction has been established. In the palliative setting to alleviate central airway obstruction, the use of laser resection, electrocautery, argon plasma coagulation, photodynamic therapy and cryotherapy can provide relief of an airway obstruction. Cryotherapy is the therapeutic application of extreme cold for the local destruction of living tissue. Recently, this technique has been used for endoscopic management of central airway obstructions in Korea. We report the role and complications of the use of cryotherapy for airway obstructions in patients with advanced lung cancer.
METHODS
We used a flexible cryoprobe for cryotherapy using nitrous oxide as a cryogen. The cryoprobe was applied through the working channel of a flexible fiberoptic bronchoscope. The temperature of the tip was approximately -89degrees C, and the icing time was 5~20 seconds.
RESULTS
Four patients with a central airway obstruction from advanced lung cancer were treated with cryotherapy. Three of the four patients were treated successfully and the airway obstruction was improved after the cryotherapy procedure. Dyspnea, hypoxia and atelectais were improved in three cases. Two patients experienced complications-one patient experienced pneumomediastinum and the other patient experienced massive hemoptysis during the cryotherapy procedure. However, these complications resolved and did not influence mortality.
CONCLUSION
This technique is effective and relatively safe for palliation of inoperable advanced lung cancer with a central airway obstruction.
Keyword
MeSH Terms
Figure
-
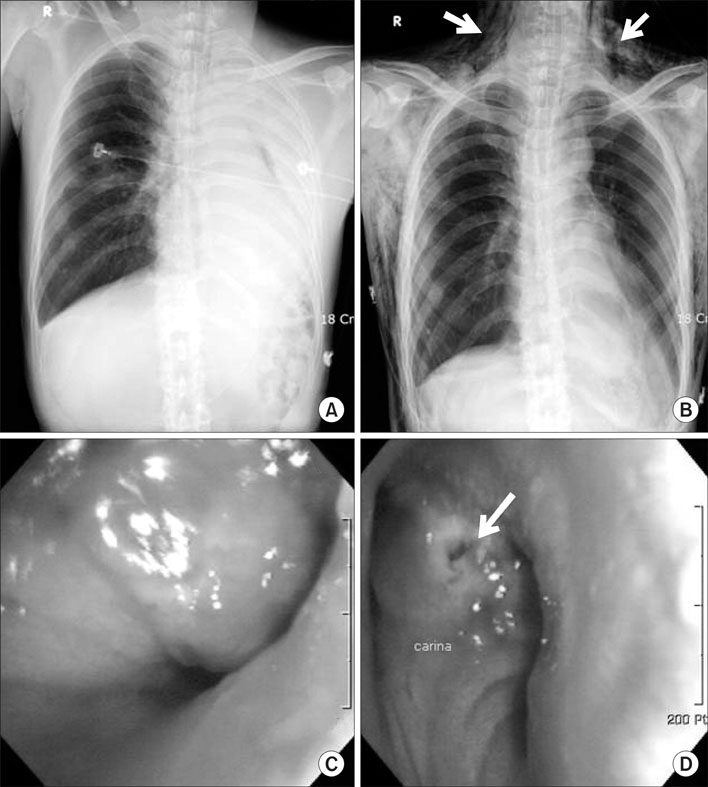
Figure 1 The chest PA and bronchoscopic finding before (A, C) and after (B, D) cryotherapy in case 2. The chest PA shows near completely obstructed left main bronchus and atelectasis of left lung. After cryotherapy, atelectasis of left lung was completely recovered, however pneumomediastinum and subcutaneous emphysema were developed (B, arrow). Bronchoscopic finding shows perforated carina after cryotherapy (D, arrow).
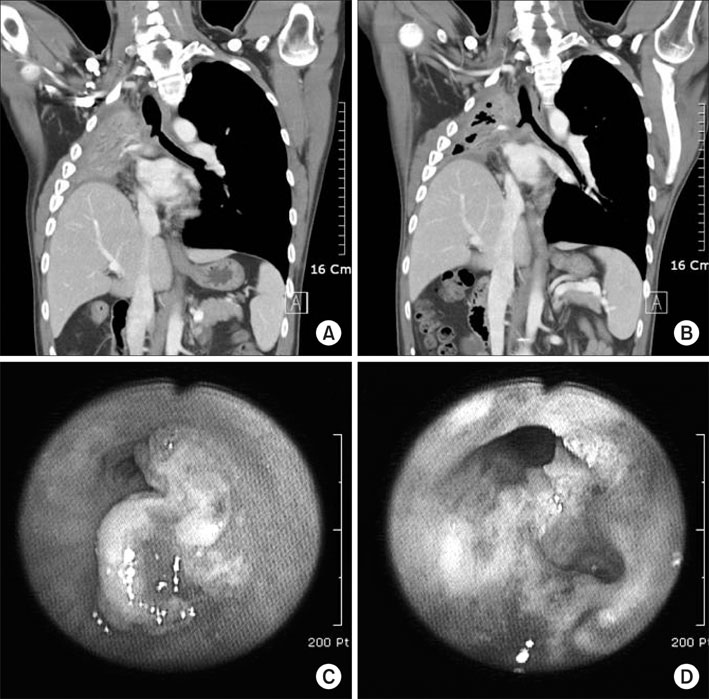
Figure 2 The chest PA and bronchoscopic finding before (A, C) and after (B, D) cryotherapy in case 3. The right main bronchus was completely obstructed by the intraluminal ingrowing tumor lesion that was extending to the distal trachea and developed severe airway obstruction (A, C). The ingrowing tumor lesion was disappeared by cryotherapy and also some aeration was noted on right upper area in chest CT scan (B, D).
Reference
-
1. Maiwand MO, Homasson JP. Cryotherapy for tracheobronchial disorders. Clin Chest Med. 1995. 16:427–443.2. Chetty KG, Moran EM, Sassoon CS, Viravathana T, Light RW. Effect of radiation therapy on bronchial obstruction due to bronchogenic carcinoma. Chest. 1989. 95:582–584.3. Sguazzi A, Bracco D. A historical account of the technical means used in cryotherapy. Minerva Med. 1974. 65:3718–3722.4. Arnott J. On the present state of therapeutic enquiry. 1845. London:5. Neel HB 3rd, Farrell KH, DeSanto LW, Payne WS, Sanderson DR. Cryosurgery of respiratory structures. I. Cryonecrosis of trachea and bronchus. Laryngoscope. 1973. 83:1062–1071.6. Homasson JP, Renault P, Angebault M, Bonniot JP, Bell NJ. Bronchoscopic cryotherapy for airway strictures caused by tumors. Chest. 1986. 90:159–164.7. Rubinsky B, Ikeda M. A cryomicroscope using directional solidification for the controlled freezing of biological material. Cryobiology. 1985. 22:55–68.8. Mazur P. Cryobiology: the freezing of biological systems. Science. 1970. 168:939–949.9. Rubinsky B, Lee CY, Bastacky J, Onik G. The process of freezing and the mechanism of damage during hepatic cryosurgery. Cryobiology. 1990. 27:85–97.10. Sheski FD, Mathur PN. Cryotherapy, electrocautery, and brachytherapy. Clin Chest Med. 1999. 20:123–138.11. Kvale PA, Selecky PA, Prakash UB. Palliative care in lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007. 132:368S–403S.12. Cavaliere S, Venuta F, Foccoli P, Toninelli C, La Face B. Endoscopic treatment of malignant airway obstructions in 2,008 patients. Chest. 1996. 110:1536–1542.13. Vergnon JM, Huber RM, Moghissi K. Place of cryotherapy, brachytherapy and photodynamic therapy in therapeutic bronchoscopy of lung cancers. Eur Respir J. 2006. 28:200–218.14. Chan AL, Yoneda KY, Allen RP, Albertson TE. Advances in the management of endobronchial lung malignancies. Curr Opin Pulm Med. 2003. 9:301–308.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Central Airway Obstruction Treated with an Insulation-Tipped Diathermic Knife-2
- Covered Bronchial Stent Insertion to Manage Airway Obstruction with Hemoptysis Caused by Lung Cancer
- Bronchoscopic Cryotherapy in Patients with Central Airway Obstruction
- Radiation Effect on Airway Obstruction from Lung Cancer
- Clinical Outcomes of Bronchoscopic Cryotherapy for Central Airway Obstruction in Adults: An 11-Years’ Experience of a Single Center
