Easy sedation anesthesia guide for non-anesthetic medical personnel
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Korea University Ansan Hospital, Ansan, Korea. minware2@korea.ac.kr
- KMID: 2467984
- DOI: http://doi.org/10.5124/jkma.2020.63.1.36
Abstract
- Currently, sedation anesthesia is increasingly used in many medical fields, from gastroscopy to medical imaging. The demand for sedation anesthesia is expected to increase gradually with increasing number of day surgeries and increased expectations from medical services. The demand for sedation anesthesia is considerably higher than the available pool of anesthesiologists; therefore, in a significant number of cases, sedation anesthesia is induced by non-anesthesiologists. However, there is no systematic provision of education or expertise for non-anesthesiologists in delivering sedation anesthesia. In cases of non-anesthesiologists inducing anesthesia, social controversy is often caused by medical accidents and substance abuse. In this review, I have briefly summarized what non-anesthesiologists should know about sedation anesthesia and have presented guidelines simplifying sedation anesthesia for non-anesthesia medical personnel.
Keyword
MeSH Terms
Figure
-

Figure 1. Modified Mallampati classification. Class I: soft palate, fauces, uvula, pillars are visible. Class II: soft palate, fauces, the part of uvula are visible. Class III: soft palate, the bottom of uvula are visible. Class IV: only hard palate is visible. Bair AE, Caravelli R, Tyler K, Laurin EG. Feasibility of the preoperative Mallampati airway assessment in emergency department patients. J Emerg Med 2010;38:677-680. Illustration by Min TJ.

Figure 2. Anesthetic depth measuring systems. (A) Bispectral index, (B) entropy, (C) schematic diagram for sedation depth, and (D) autonomic indicators.
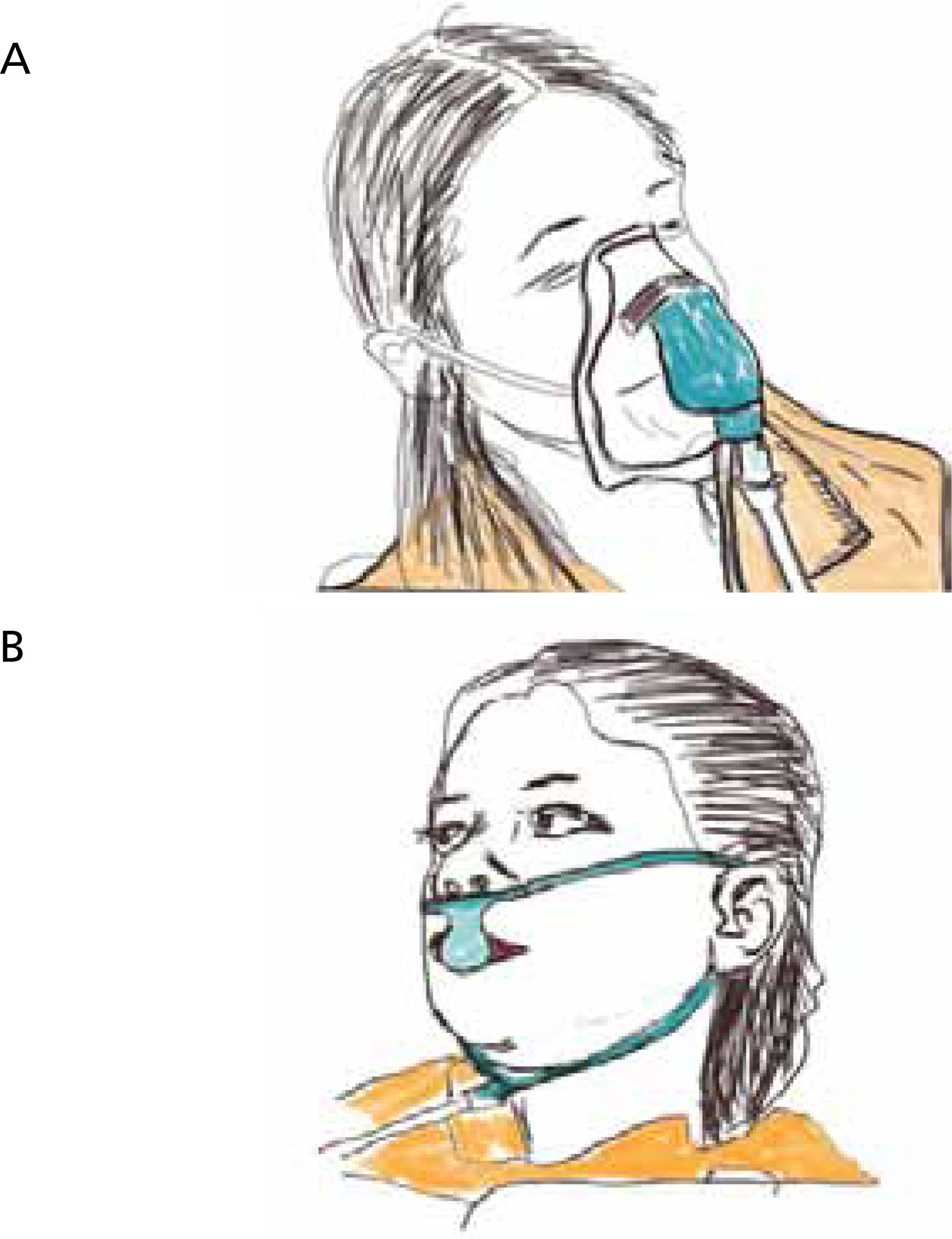
Figure 3. End-tidal CO2 monitoring device. (A) Mask end-tidal CO2 monitoring device. (B) Nasal prong end-tidal CO2 monitoring device. Illustration by Min TJ.

Figure 4. Airway secure maneuvers. (A) Head tilt chin-lift maneuver. (B) Jaw-thrust maneuver. Pratice Paramedicine, July 5, 2018. Illustration by Min TJ.

Figure 5. Airway secure devices. (A) Oral airway. (B) Nasal airway. (C) Laryngeal mask.
Reference
-
1. Solomon SA, Kajla VK, Banerjee AK. Can the elderly tolerate endoscopy without sedation? J R Coll Physicians Lond. 1994; 28:407–410.2. Schutz SM, Lee JG, Schmitt CM, Almon M, Baillie J. Clues to patient dissatisfaction with conscious sedation for colonoscopy. Am J Gastroenterol. 1994; 89:1476–1479.3. American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002; 96:1004–1017.4. Dewdney C, MacDougall M, Blackburn R, Lloyd G, Gray A. Capnography for procedural sedation in the ED: a systematic review. Emerg Med J. 2017; 34:476–484.
Article5. Addison PS. A review of signal processing used in the implementation of the pulse oximetry photoplethysmographic fluid responsiveness parameter. Anesth Analg. 2014; 119:1293–1306.
Article6. Polster MR, Gray PA, OʼSullivan G, McCarthy RA, Park GR. Comparison of the sedative and amnesic effects of midazolam and propofol. Br J Anaesth. 1993; 70:612–616.
Article7. Shafer SL. Advances in propofol pharmacokinetics and pharmacodynamics. J Clin Anesth. 1993; 5(6 Suppl 1):14S–21S.
Article8. Barr J, Egan TD, Sandoval NF, Zomorodi K, Cohane C, Gambus PL, Shafer SL. Propofol dosing regimens for ICU sedation based upon an integrated pharmacokinetic-pharmacodynamic model. Anesthesiology. 2001; 95:324–333.9. Fellows IW, Byrne AJ, Allison SP. Adrenocortical suppression with etomidate. Lancet. 1983; 2:54–55.
Article10. Venn RM, Karol MD, Grounds RM. Pharmacokinetics of dexmedetomidine infusions for sedation of postoperative patients requiring intensive caret. Br J Anaesth. 2002; 88:669–675.11. Tan JA, Ho KM. Use of dexmedetomidine as a sedative and analgesic agent in critically ill adult patients: a metaanalysis. Intensive Care Med. 2010; 36:926–939.
Article12. Maze M, Scarfini C, Cavaliere F. New agents for sedation in the intensive care unit. Crit Care Clin. 2001; 17:881–897.
Article13. Okamoto GU, Duperon DF, Jedrychowski JR. Clinical evaluation of the effects of ketamine sedation on pediatric dental patients. J Clin Pediatr Dent. 1992; 16:253–257.14. Min JY, Lee JR, Kim HI, Byon HJ. Factors affecting determination of the optimal ketamine dose for pediatric sedation. Clin Exp Emerg Med. 2019; 6:119–124.
Article15. Yang TY, Lee TK, Choi JH, Woo SH. Non-general anesthesia for the correction of pediatric trigger thumbs. Arch Hand Microsurg. 2019; 24:10–16.
Article16. Slavik VC, Zed PJ. Combination ketamine and propofol for procedural sedation and analgesia. Pharmacotherapy. 2007; 27:1588–1598.
Article17. Egan TD, Huizinga B, Gupta SK, Jaarsma RL, Sperry RJ, Yee JB, Muir KT. Remifentanil pharmacokinetics in obese versus lean patients. Anesthesiology. 1998; 89:562–573.
Article18. Kim HS, Baek SY, Park DH, Ryu KH. Use of remifentanil and propofol without muscle relaxant with Duchenne muscular dystrophy: a case report. Anesth Pain Med. 2018; 13:30–33.19. Hwang J, Shin JS, Son JH, Min TJ. Non-intubated thoracoscopic bullectomy under sedation is safe and comfortable in the perioperative period. J Thorac Dis. 2018; 10:1703–1710.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthesia and Sedation
- Anesthetic Experience of Spinal Anesthesia after Sedation in Un-cooperated Elderly Patients
- Procedural sedation and analgesia in pediatric emergency department
- Monitored Anesthesia Care and Sedation/Analgesia Outside the Operating Room
- Sedation for routine gastrointestinal endoscopic procedures: a review on efficacy, safety, efficiency, cost and satisfaction
