Protective effect of glucosamine and risedronate (alone or in combination) against osteoarthritic changes in rat experimental model of immobilized knee
- Affiliations
-
- 1Department of Anatomy, Faculty of Medicine, Menoufia University, Al Minufya, Egypt. Ahmedsalman1971@gmail.com
- 2Department of Anatomy and Histology, Faculty of Medicine, The University of Jordan, Amman, Jordan.
- 3Department of Anatomy, Faculty of Medicine, Ain Shams University, Cairo, Egypt.
- 4Department of Anatomy, Faculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia.
- 5Department of Histology, Faculty of Medicine, Menoufia University, Al Minufya, Egypt.
- KMID: 2466704
- DOI: http://doi.org/10.5115/acb.19.050
Abstract
- This study is aiming to investigate the protective effect of glucosamine, risedronate (alone or in combination) on articular cartilage in experimental model of immobilized rat knee. Twenty-five adult male albino rats were divided into five groups (five rats each): control group, immobilized group, glucosamine-treated group, risedronate-treated group, and group treated by a combination of glucosamine and risedronate. The articular cartilage was obtained for histological, immunohistochemical and morphometric studies. The immobilized group showed manifestations of osteoarthritis in the form of significant decrease of articular cartilage thickness with surface erosions, shrunken chondrocytes with pyknotic nuclei and marked manifested fall of chondrocyte number. There was manifested reduction of collagen contents of the articular cartilage using Masson trichrome stain. Safranin O-Fast Green revealed low proteoglycan contents. The collagen type II was also declined. The manikin score was 7.8. Risedronate improved this manifestation slightly more than glucosamine, but combination of booth drugs caused significant improvement of the damaged articular cartilage caused by immobilization. Oral administration of glucosamine and risedronate improved the degenerative changes of rat knee articular cartilage that follow immobilization. This improvement was more remarkable when both drugs were used in combination.
Keyword
MeSH Terms
Figure
-
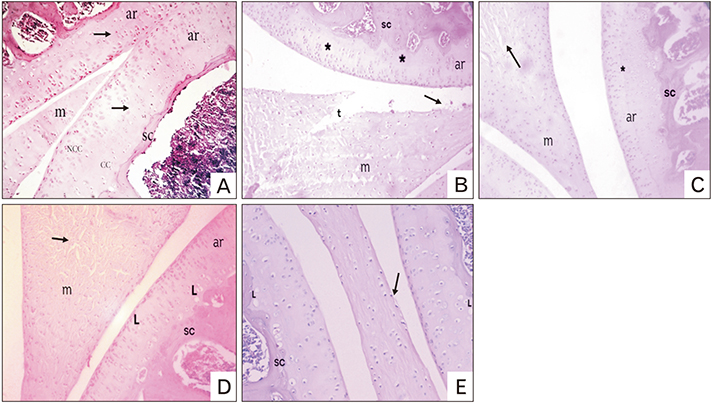
Fig. 1 Hematoxylin and eosin (H&E)–stained sections of the knee joint of different groups. (A) Control group showing articular cartilage with regular smooth intact surface and well-organized chondrocytes which appeared in non-calcified (NCC) and calcified (CC) regions of cartilage with a clear intact tidemark (arrows) in between. The subchondral bone (SC) appears intact. The meniscus shows regular smooth surface with no fraying or undulation. (B) Immobilized group showing reduction in thickness of articular cartilage, shrunken chondrocytes, absence of chondrocytes in some areas (*) and invisible tidemark. The SC appears intact. Meniscus shows severe fraying and tears and erosion of surface with necrotic cells shedding from it (arrow). (C) The immobilized group treated with glucosamine; the articular cartilage shows smooth surface, shrunken chondrocytes and visible tidemark (*). The SC appears intact. The meniscus shows smooth surface with some cracks (arrow). (D) The immobilized group treated with risedronate; the articular cartilage shows smooth surface, shrunken chondrocytes, some empty lacunae, and hardly visible tidemark. The SC appears intact. The meniscus shows smooth surface with some cracks (arrow). (E) immobilized group treated with glucosamine and risedronate; the articular cartilage shows smooth surface, few shrunken chondrocytes, some empty lacunae, and visible tidemark. The SC appears intact. The meniscus shows minimal erosion of its surface (arrow) (H&E, ×200). ar, articular cartilage; L, lacunae; m, meniscus; t, tears.
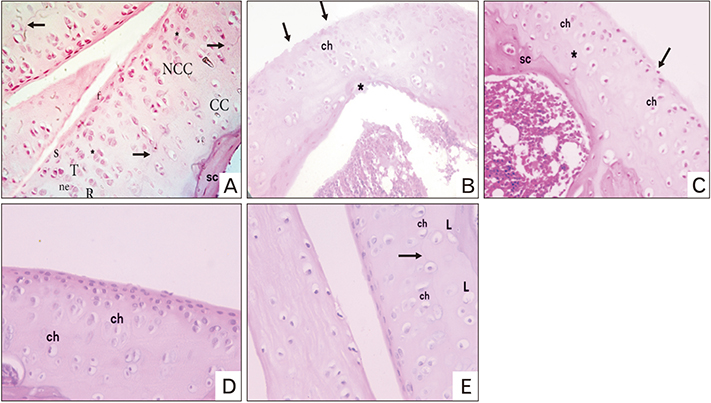
Fig. 2 Hematoxylin and eosin (H&E)–stained sections of articular cartilage of knee joint of different groups. (A) Control group showing the chondrocytes in non-calcified region (NCC) of the articular cartilage arranged in three zones: superficial (S), transitional (T), and radial (R) zone. The superficial zone contains small flat chondrocytes. The transitional and radial zone contain columns of rounded, oval, or triangular chondrocytes (*). The chondrocytes are located inside their lacunae forming cell nests. The calcified region (CC) is separated from radial zone by a tidemark (arrows). The subchondral bone (SC) appears intact. (B) Immobilized group; articular cartilage shows irregular notched surface (arrows) and its chondrocytes appear shrunken with pyknotic nuclei, disorganized and few in number. Tidemark is invisible. The subchondral bone shows degenerative changes (*). (C) The immobilized group treated with glucosamine; articular cartilage shows irregular degenerated surface (arrow) and shrunken chondrocytes which appear disorganized and few in number. Tidemark is visible. The SC appears intact. (D) The immobilized group treated with risedronate; articular cartilage shows smooth surface, shrunken chondrocytes which appear disorganized and few in number. Tidemark is not clearly visible. (E) The immobilized group treated with glucosamine and risedronate; articular cartilage shows smooth surface, few shrunken chondrocytes, few empty lacunae, and visible tidemark (arrow) (H&E, ×400). ch, chondrocyte; f, flat chondrocyte; L, lacunae; ne, cell nests.
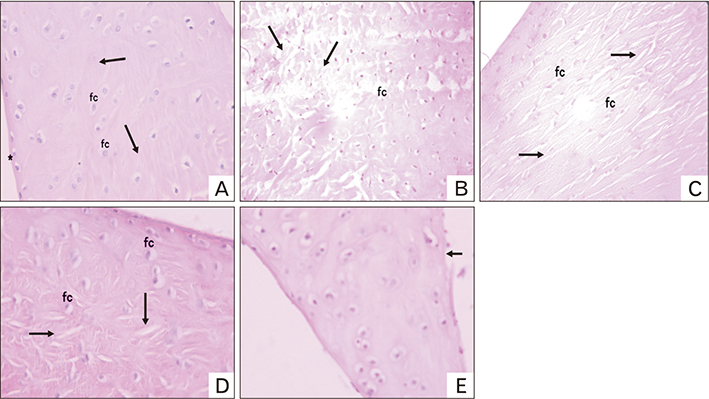
Fig. 3 Hematoxylin and eosin–stained sections of meniscus of the knee joint of different groups. (A) Control group showing the meniscus composed of homogenous eosinophilic staining well-organized collagen fibers (arrows) with fibrochondrocytes in their lacunae. The meniscus surface is smooth with no fraying or undulation (*). (B) Immobilized group showing many meniscal tears with unorganized disrupted collagen fibers (arrows) and markedly shrunken darkly stained fibrochondrocytes. (C) The immobilized group treated with glucosamine showing some tears and cracks (arrows) and moderately shrunken darkly stained fibrochondrocytes. (D) The immobilized group treated with risedronate showing few tears and cracks (arrows) and slightly shrunken fibrochondrocytes. (E) The immobilized group treated with glucosamine and risedronate showing nearly normal meniscus except for minimal erosion of its surface (arrow) (H&E, ×400). fc, fibrochondrocytes.
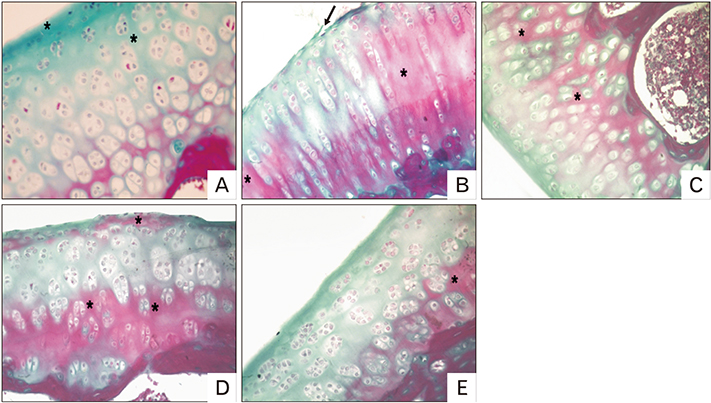
Fig. 4 A photomicrograph of Masson trichrome–stained sections of articular cartilage of knee joint of different groups. (A) Control group showing the articular cartilage which is well stained with Masson trichrome for collagen (green color) (*). (B) Immobilized group showing marked reduction of Masson trichrome–stained area for collagen with appearance of an extensive red color (*). Minimal erosion of the articular cartilage surface is observed (arrow). (C) The immobilized group treated with glucosamine showing marked reduction of Masson trichrome–stained area for collagen with appearance of a red color (*). (D) The immobilized group treated with risedronate showing moderate reduction of Masson trichrome–stained area for collagen with appearance of a red color (*). (E) The immobilized group treated with glucosamine and risedronate showing slight reduction of Masson trichrome–stained area for collagen with appearance of a slight red color (*) (Masson trichrome, ×400).
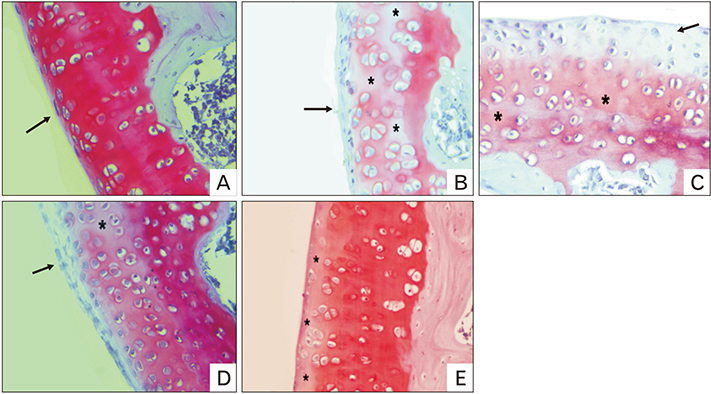
Fig. 5 A photomicrograph of Safranin O–Fast Green (SO)–stained sections of articular cartilage of knee joint of different groups. (A) Control group showing the articular cartilage which appears well stained with SO. The smooth surface of the articular cartilage (arrow) with normal cellular distribution is observed. (B) Immobilized group showing marked reduction in SO staining intensity in the non-calcified region of the articular cartilage (*) and slight reduction in its calcified region. The surface of articular cartilage shows fibrillation (arrow). (C) The immobilized group treated with glucosamine showing marked reduction in SO staining intensity in the superficial part (arrow) of the articular cartilage and moderate reduction in its deeper part (*). The smooth surface of the articular cartilage is observed. (D) The immobilized group treated with risedronate showing moderate reduction in SO staining intensity in the calcified region of the articular cartilage (*) with disruption in the superficial part of the articular cartilage (arrow). (E) The immobilized group treated with glucosamine and risedronate showing slight reduction in SO staining intensity in the superficial part of the articular cartilage (*). The smooth surface of the articular cartilage is observed (SO staining, ×400).
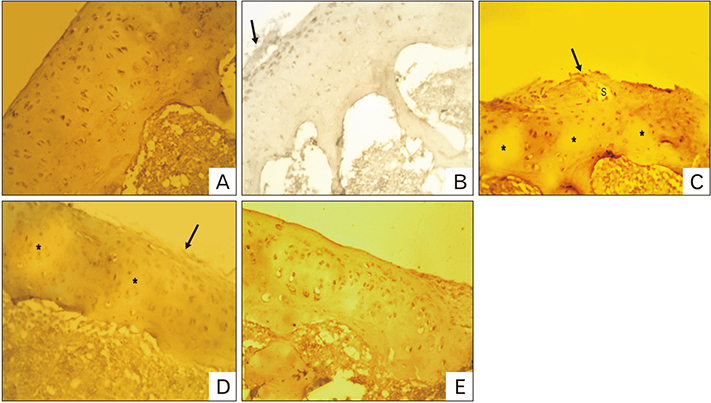
Fig. 6 Immunohistochemical stained sections for collagen type II of the articular cartilage of the knee joint of different groups. (A) Control group showing very strong immunostaining intensity for collagen type II in articular cartilage (brown color). The smooth surface of the articular cartilage is observed. (B) Immobilized group showing weak immunostaining intensity for collagen type II in articular cartilage with disruption in the superficial part of cartilage (arrow). (C) The immobilized group treated with glucosamine showing moderate immunostaining intensity for collagen type II in articular cartilage (*). Irregularity of the surface (arrow) and presence of a space in superficial part are observed. (D) The immobilized group treated with risedronate showing moderate immunostaining intensity for collagen type II in articular cartilage (*) with necrosis of superficial part of the articular cartilage (arrow). (E) The immobilized group treated with glucosamine and risedronate showing strong immunostaining intensity for collagen type II in the articular cartilage. The smooth surface of the articular cartilage is observed (immunohistochemical staining for collagen type II, ×400). s, space.
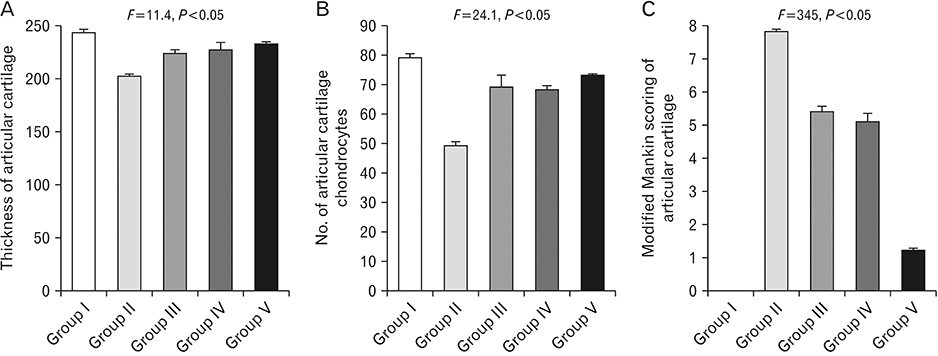
Fig. 7 (A) The thickness of the articular cartilage (µm) of different experimental groups. Pairwise significant differences were detected between: group I and group II (P<0.001); group II and group III (P<0.05), group IV (P<0.01) and group V (P<0.001); group III and groups IV and V (P>0.05); group IV and group V (P>0.05). (B) The number of the chondrocytes in the articular cartilage of different experimental groups. Pairwise significant differences were detected between: group I and group II (P<0.001); group II and groups III, IV and V (P<0.001); group III and groups IV and V (P>0.05); group IV and group V (P>0.05). (C) The number of the chondrocytes in the articular cartilage of different experimental groups. Pairwise significant differences were detected between: group I and group II (P<0.001); group II and groups III, IV, and V (P<0.001); group III and group IV (P>0.05), V (P<0.001); group IV and group V (P<0.001). Group I, control; group II, immobilized knee; group III, immobilized group treated with glucosamine; group IV, immobilized group treated with risedronate; group V, immobilized group treated with glucosamine and risedronate. Analysis was done using GraphPad Prism version 4. Data were analyzed by using one-way analysis of variance test followed by Bonferroni's multiple comparison post-hoc test for comparison between all groups. P>0.05, nonsignificant; P<0.05, significant.
Reference
-
1. Iqbal K, Khan Y, Minhas LA. Effects of immobilization on thickness of superficial zone of articular cartilage of patella in rats. Indian J Orthop. 2012; 46:391–394.2. Eyre D. Collagen of articular cartilage. Arthritis Res. 2002; 4:30–35.3. Hunter W. Of the structure and disease of articulating cartilages. 1743. Clin Orthop Relat Res. 1995; (317):3–6.4. Newman AP. Articular cartilage repair. Am J Sports Med. 1998; 26:309–324.5. Sprouse RA, McLaughlin AM, Harris GD. Braces and splints for common musculoskeletal conditions. Am Fam Physician. 2018; 98:570–576.6. Buckwalter JA. Osteoarthritis and articular cartilage use, disuse, and abuse: experimental studies. J Rheumatol Suppl. 1995; 43:13–15.7. Setton LA, Mow VC, Muller FJ, Pita JC, Howell DS. Mechanical behavior and biochemical composition of canine knee cartilage following periods of joint disuse and disuse with remobilization. Osteoarthritis Cartilage. 1997; 5:1–16.8. Jurvelin J, Kiviranta I, Tammi M, Helminen JH. Softening of canine articular cartilage after immobilization of the knee joint. Clin Orthop Relat Res. 1986; (207):246–252.9. Hagiwara Y, Ando A, Chimoto E, Saijo Y, Ohmori-Matsuda K, Itoi E. Changes of articular cartilage after immobilization in a rat knee contracture model. J Orthop Res. 2009; 27:236–242.10. Mosekilde L, Thomsen JS, Mackey MS, Phipps RJ. Treatment with risedronate or alendronate prevents hind-limb immobilization-induced loss of bone density and strength in adult female rats. Bone. 2000; 27:639–645.11. Towheed TE, Maxwell L, Anastassiades TP, Shea B, Houpt J, Robinson V, Hochberg MC, Wells G. Glucosamine therapy for treating osteoarthritis. Cochrane Database Syst Rev. 2005; (2):CD002946.12. Shikhman AR, Amiel D, D'Lima D, Hwang SB, Hu C, Xu A, Hashimoto S, Kobayashi K, Sasho T, Lotz MK. Chondroprotective activity of N-acetylglucosamine in rabbits with experimental osteoarthritis. Ann Rheum Dis. 2005; 64:89–94.13. Tiraloche G, Girard C, Chouinard L, Sampalis J, Moquin L, Ionescu M, Reiner A, Poole AR, Laverty S. Effect of oral glucosamine on cartilage degradation in a rabbit model of osteoarthritis. Arthritis Rheum. 2005; 52:1118–1128.14. Pavelká K, Gatterová J, Olejarová M, Machacek S, Giacovelli G, Rovati LC. Glucosamine sulfate use and delay of progression of knee osteoarthritis: a 3-year, randomized, placebo-controlled, double-blind study. Arch Intern Med. 2002; 162:2113–2123.15. Herrero-Beaumont G, Ivorra JA, Del Carmen, Blanco FJ, Benito P, Martin-Mola E, Paulino J, Marenco JL, Porto A, Laffon A, Araújo D, Figueroa M, Branco J. Glucosamine sulfate in the treatment of knee osteoarthritis symptoms: a randomized, double-blind, placebo-controlled study using acetaminophen as a side comparator. Arthritis Rheum. 2007; 56:555–567.16. Bruyere O, Pavelka K, Rovati LC, Deroisy R, Olejarova M, Gatterova J, Giacovelli G, Reginster JY. Glucosamine sulfate reduces osteoarthritis progression in postmenopausal women with knee osteoarthritis: evidence from two 3-year studies. Menopause. 2004; 11:138–143.17. da Camara CC, Dowless GV. Glucosamine sulfate for osteoarthritis. Ann Pharmacother. 1998; 32:580–587.18. Spector TD, Conaghan PG, Buckland-Wright JC, Garnero P, Cline GA, Beary JF, Valent DJ, Meyer JM. Effect of risedronate on joint structure and symptoms of knee osteoarthritis: results of the BRISK randomized, controlled trial [ISRCTN01928173]. Arthritis Res Ther. 2005; 7:R625–R633.19. Garnero P, Aronstein WS, Cohen SB, Conaghan PG, Cline GA, Christiansen C, Beary JF, Meyer JM, Bingham CO 3rd. Relationships between biochemical markers of bone and cartilage degradation with radiological progression in patients with knee osteoarthritis receiving risedronate: the Knee Osteoarthritis Structural Arthritis randomized clinical trial. Osteoarthritis Cartilage. 2008; 16:660–666.20. Doschak MR, Wohl GR, Hanley DA, Bray RC, Zernicke RF. Antiresorptive therapy conserves some periarticular bone and ligament mechanical properties after anterior cruciate ligament disruption in the rabbit knee. J Orthop Res. 2004; 22:942–948.21. Spector TD. Bisphosphonates: potential therapeutic agents for disease modification in osteoarthritis. Aging Clin Exp Res. 2003; 15:413–418.22. Jones MD, Tran CW, Li G, Maksymowych WP, Zernicke RF, Doschak MR. In vivo microfocal computed tomography and micro-magnetic resonance imaging evaluation of antiresorptive and antiinflammatory drugs as preventive treatments of osteoarthritis in the rat. Arthritis Rheum. 2010; 62:2726–2735.23. Aghazadeh-Habashi A, Kohan MH, Asghar W, Jamali F. Glucosamine dose/concentration-effect correlation in the rat with adjuvant arthritis. J Pharm Sci. 2014; 103:760–767.24. Nakabayashi K, Sakamoto J, Kataoka H, Kondo Y, Hamaue Y, Honda Y, Nakano J, Okita M. Effect of continuous passive motion initiated after the onset of arthritis on inflammation and secondary hyperalgesia in rats. Physiol Res. 2016; 65:683–691.25. Tuukkanen J, Peng Z, Väänänen HK. The effect of training on the recovery from immobilization-induced bone loss in rats. Acta Physiol Scand. 1992; 145:407–411.26. Roberts S, McCall IW, Darby AJ, Menage J, Evans H, Harrison PE, Richardson JB. Autologous chondrocyte implantation for cartilage repair: monitoring its success by magnetic resonance imaging and histology. Arthritis Res Ther. 2003; 5:R60–R73.27. Mankin HJ, Dorfman H, Lippiello L, Zarins A. Biochemical and metabolic abnormalities in articular cartilage from osteo-arthritic human hips. II. Correlation of morphology with biochemical and metabolic data. J Bone Joint Surg Am. 1971; 53:523–537.28. Gault SJ, Spyker MJ. Beneficial effect of immobilization of joints in rheumatoid and related arthritides: a splint study using sequential analysis. Arthritis Rheum. 1969; 12:34–44.29. Säämänen AM, Tammi M, Kiviranta I, Jurvelin J, Helminen HJ. Maturation of proteoglycan matrix in articular cartilage under increased and decreased joint loading: a study in young rabbits. Connect Tissue Res. 1987; 16:163–175.30. Evans EB, Eggers GW, Butler JK, Blumel J. Experimental immobilization and remobilization of rat knee joints. J Bone Joint Surg. 1960; 42:737–758.31. Hall MC. Cartilage changes after experimental immobilization of the knee joint of the young rat. J Bone Joint Surg. 1963; 45:36–44.32. Trudel G, Himori K, Uhthoff HK. Contrasting alterations of apposed and unapposed articular cartilage during joint contracture formation. Arch Phys Med Rehabil. 2005; 86:90–97.33. Akeson WH, Amiel D, Woo SL. Immobility effects on synovial joints the pathomechanics of joint contracture. Biorheology. 1980; 17:95–110.34. Videman T. Experimental osteoarthritis in the rabbit: comparison of different periods of repeated immobilization. Acta Orthop Scand. 1982; 53:339–347.35. Iqbal K, Khan MY, Minhas LA. Effects of immobilisation and remobilisation on superficial zone of articular cartilage of patella in rats. J Pak Med Assoc. 2012; 62:531–535.36. Tammi M, Saamanen AM, Jauhiainen A, Malminen O, Kiviranta I, Helminen H. Proteoglycan alterations in rabbit knee articular cartilage following physical exercise and immobilization. Connect Tissue Res. 1983; 11:45–55.37. Palmoski MJ, Brandt KD. Running inhibits the reversal of atrophic changes in canine knee cartilage after removal of a leg cast. Arthritis Rheum. 1981; 24:1329–1337.38. Behrens F, Kraft EL, Oegema TR Jr. Biochemical changes in articular cartilage after joint immobilization by casting or external fixation. J Orthop Res. 1989; 7:335–343.39. Haapala J, Arokoski JP, Hyttinen MM, Lammi M, Tammi M, Kovanen V, Helminen HJ, Kiviranta I. Remobilization does not fully restore immobilization induced articular cartilage atrophy. Clin Orthop Relat Res. 1999; (362):218–229.40. Aldahmash AM, El Fouhil AF, Mohamed RA, Ahmed AM, Atteya M, Al Sharawy SA, Qureshi RA. Collagen types I and II distribution: a relevant indicator for the functional properties of articular cartilage in immobilised and remobilized rabbit knee joints. Folia Morphol (Warsz). 2015; 74:169–175.41. Narmoneva DA, Cheung HS, Wang JY, Howell DS, Setton LA. Altered swelling behavior of femoral cartilage following joint immobilization in a canine model. J Orthop Res. 2002; 20:83–91.42. Videman T, Michelsson JE, Langenskiold A. The development of radiographic changes in experimental osteoarthritis provoked by immobilization of the knee in rabbits. Int Res Commun Syst Med Sci. 1977; 5:62.43. Videman T, Eronen I, Friman C, Langenskiöld A. Glycosaminoglycan metabolism of the medial meniscus, the medial collateral ligament and the hip joint capsule in experimental osteoarthritis caused by immobilization of the rabbit knee. Acta Orthop Scand. 1979; 50:465–470.44. Thaxter TH, Mann RA, Anderson CE. Degeneration of immobilized knee joints in rats: histological and autoradiographic study. J Bone Joint Surg Am. 1965; 47:567–585.45. Maldonado DC, Silva MC, Neto Sel-R, de Souza MR, de Souza RR. The effects of joint immobilization on articular cartilage of the knee in previously exercised rats. J Anat. 2013; 222:518–525.46. Kiviranta I, Tammi M, Jurvelin J, Arokoski J, Säämänen AM, Helminen HJ. Articular cartilage thickness and glycosaminoglycan distribution in the young canine knee joint after remobilization of the immobilized limb. J Orthop Res. 1994; 12:161–167.47. Sood SC. A study of the effects of experimental immobilisation on rabbit articular cartilage. J Anat. 1971; 108(Pt 3):497–507.48. O'Connor KM. Unweighting accelerates tidemark advancement in articular cartilage at the knee joint of rats. J Bone Miner Res. 1997; 12:580–589.49. Leroux MA, Cheung HS, Bau JL, Wang JY, Howell DS, Setton LA. Altered mechanics and histomorphometry of canine tibial cartilage following joint immobilization. Osteoarthritis Cartilage. 2001; 9:633–640.50. Gyarmati J, Foldes I, Kern M, Kiss I. Morphological studies on the articular cartilage of old rats. Acta Morphol Hung. 1987; 35:111–124.51. Tammi M, Kiviranta I, Peltonen L, Jurvelin J, Helminen HJ. Effects of joint loading on articular cartilage collagen metabolism: assay of procollagen prolyl 4-hydroxylase and galactosylhydroxylysyl glucosyltransferase. Connect Tissue Res. 1988; 17:199–206.52. Videman T, Eronen I, Candolin T. [3H]proline incorporation and hydroxyproline concentration in articular cartilage during the development of osteoarthritis caused by immobilization. A study in vivo with rabbits. Biochem J. 1981; 200:435–440.53. Muller FJ, Setton LA, Manicourt DH, Mow VC, Howell DS, Pita JC. Centrifugal and biochemical comparison of proteoglycan aggregates from articular cartilage in experimental joint disuse and joint instability. J Orthop Res. 1994; 12:498–508.54. Haapala J, Arokoski J, Pirttimaki J, Lyyra T, Jurvelin J, Tammi M, Helminen HJ, Kiviranta I. Incomplete restoration of immobilization induced softening of young beagle knee articular cartilage after 50-week remobilization. Int J Sports Med. 2000; 21:76–81.55. Jortikka MO, Inkinen RI, Tammi MI, Parkkinen JJ, Haapala J, Kiviranta I, Helminen HJ, Lammi MJ. Immobilisation causes longlasting matrix changes both in the immobilised and contralateral joint cartilage. Ann Rheum Dis. 1997; 56:255–261.56. Mow VC, Proctor CS, Kelly MA. Biomechanics of articular cartilage. In : Nordin M, Frankel VH, editors. Basic Biomechanics of the Musculoskeletal System. 2nd ed. London: Lea & Febiger;1989. p. 31–58.57. Cawston TE, Wilson AJ. Understanding the roleof tissue degrading enzymes and their inhibitors in development and disease. Best Pract Res Clin Rheumatol. 2006; 20:983–1002.58. Echtermeyer F, Bertrand J, Dreier R, Meinecke I, Neugebauer K, Fuerst M, Lee YJ, Song YW, Herzog C, Theilmeier G, Pap T. Syndecan-4 regulates ADAMTS-5 activation and cartilage breakdown in osteoarthritis. Nat Med. 2009; 15:1072–1076.59. Lohmander LS, Hoerrner LA, Dahlberg L, Roos H, Björnsson S, Lark MW. Stromelysin, tissue inhibitor of metalloproteinases and proteoglycan fragments in human knee joint fluid after injury. J Rheumatol. 1993; 20:1362–1368.60. Walakovits LA, Moore VL, Bhardwaj N, Gallick GS, Lark MW. Detection of stromelysin and collagenase in synovial fluid from patients with rheumatoid arthritis and posttraumatic knee injury. Arthritis Rheum. 1992; 35:35–42.61. Grumbles RM, Howell DS, Howard GA, Roos BA, Setton LA, Mow VC, Ratcliffe A, Muller FJ, Altman RD. Cartilage metalloproteases in disuse atrophy. J Rheumatol Suppl. 1995; 43:146–148.62. Leong DJ, Gu XI, Li Y, Lee JY, Laudier DM, Majeska RJ, Schaffler MB, Cardoso L, Sun HB. Matrix metalloproteinase-3 in articular cartilage is upregulated by joint immobilization and suppressed by passive joint motion. Matrix Biol. 2010; 29:420–426.63. Helminen HJ, Jurvelin J, Kuusela T, Heikkilä R, Kiviranta I, Tammi M. Effects of immobilization for 6 weeks on rabbit knee articular surfaces as assessed by the semiquantitative stereomicroscopic method. Acta Anat (Basel). 1983; 115:327–335.64. Kiviranta I, Jurvelin J, Tammi M, Säämänen AM, Helminen HJ. Weight bearing controls glycosaminoglycan concentration and articular cartilage thickness in the knee joints of young beagle dogs. Arthritis Rheum. 1987; 30:801–809.65. Reginster JY, Deroisy R, Rovati LC, Lee RL, Lejeune E, Bruyere O, Giacovelli G, HenrotinY , Dacre JE, Gossett C. Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. Lancet. 2001; 357:251–256.66. Vidal y Plana RR, Bizzarri D, Rovati AL. Articular cartilage pharmacology: I. In vitro studies on glucosamine and non steroidal antiinflammatory drugs. Pharmacol Res Commun. 1978; 10:557–569.67. Bassleer C, Rovati L, Franchimont P. Stimulation of proteoglycan production by glucosamine sulfate in chondrocytes isolated from human osteoarthritic articular cartilage in vitro. Osteoarthritis Cartilage. 1998; 6:427–434.68. Fenton JI, Chlebek-Brown KA, Peters TL, Caron JP, Orth MW. Glucosamine HCl reduces equine articular cartilage degradation in explant culture. Osteoarthritis Cartilage. 2000; 8:258–265.69. McCarthy G, O'Donovan J, Jones B, McAllister H, Seed M, Mooney C. Randomised double-blind, positive-controlled trial to assess the efficacy of glucosamine/chondroitin sulfate for the treatment of dogs with osteoarthritis. Vet J. 2007; 174:54–61.70. Naito K, Watari T, Furuhata A, Yomogida S, Sakamoto K, Kurosawa H, Kaneko K, Nagaoka I. Evaluation of the effect of glucosamine on an experimental rat osteoarthritis model. Life Sci. 2010; 86:538–543.71. Richy F, Bruyere O, Ethgen O, Cucherat M, Henrotin Y, Reginster JY. Structural and symptomatic efficacy of glucosamine and chondroitin in knee osteoarthritis: a comprehensive metaanalysis. Arch Intern Med. 2003; 163:1514–1522.72. Corrado A, Santoro N, Cantatore FP. Extra-skeletal effects of bisphosphonates. Joint Bone Spine. 2007; 74:32–38.73. Iwamoto J, Takeda T, Sato Y, Matsumoto H. Effects of risedronate on osteoarthritis of the knee. Yonsei Med J. 2010; 51:164–170.74. MacNeil JA, Doschak MR, Zernicke RF, Boyd SK. Preservation of periarticular cancellous morphology and mechanical stiffness in post-traumatic experimental osteoarthritis by antiresorptive therapy. Clin Biomech (Bristol, Avon). 2008; 23:365–371.75. Walker K, Medhurst SJ, Kidd BL, Glatt M, Bowes M, Patel S, McNair K, Kesingland A, Green J, Chan O, Fox AJ, Urban LA. Disease modifying and anti-nociceptive effects of the bisphosphonate, zoledronic acid in a model of bone cancer pain. Pain. 2002; 100:219–229.76. Bettica P, Cline G, Hart DJ, Meyer J, Spector TD. Evidence for increased bone resorption in patients with progressive knee osteoarthritis: longitudinal results from the Chingford study. Arthritis Rheum. 2002; 46:3178–3184.77. Brown JP, Chines AA, Myers WR, Eusebio RA, Ritter-Hrncirik C, Hayes CW. Improvement of pagetic bone lesions with risedronate treatment: a radiologic study. Bone. 2000; 26:263–267.78. Permuy M, Guede D, López-Peña M, Muñoz F, González-Cantalapiedra A, Caeiro JR. Effects of glucosamine and risedronate alone or in combination in an experimental rabbit model of osteoarthritis. BMC Vet Res. 2014; 10:97.79. Thomsen JS, Straarup TS, Danielsen CC, Oxlund H, Brüel A. No effect of risedronate on articular cartilage damage in the Dunkin Hartley guinea pig model of osteoarthritis. Scand J Rheumatol. 2013; 42:408–416.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of Glucosamine for Knee Osteoarthritis
- Effect of Carboxy Methyl Chitosan on Experimental Osteoarthritis in a Rabbit Knee: Carboxy methyl chitosan vs. Hyaluronan
- Effect of Pregnancy on Knee Joint Contracture in the Rat
- The Comparision of Mitigative Effect of Alendronate and Risedronate on Particle-Induced Osteolysis: in Mouse Calvarian Model
- The Effect of Risedronate on Posterior Lateral Spinal Fusion in a Rat Model
