Anesth Pain Med.
2018 Jan;13(1):47-52. 10.17085/apm.2018.13.1.47.
A survey of current concepts and practices related to use of neuromuscular blockers with antagonists and neuromuscular monitoring among Korean anesthesiologists
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. s2248@paik.ac.kr
- 2Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Anesthesiology and Pain Medicine, Soonchunhyang University Bucheon Hospital, Bucheon, Korea.
- KMID: 2436055
- DOI: http://doi.org/10.17085/apm.2018.13.1.47
Abstract
- BACKGROUND
The goal of this nationwide survey was to investigate the current concepts and practices of the use of neuromuscular blockers and their antagonists, and the availability and clinical practice of neuromuscular monitoring in Korea.
METHODS
After obtaining approval from the board of directors of the Korean Society of Anesthesiologists, we distributed a questionnaire via email to anesthesiology specialists with registered email addresses. The survey included questions on the availability and daily use of neuromuscular blockers, their antagonists and neuromuscular monitoring.
RESULTS
The overall response rate was 23.7%. Rocuronium and pyridostigmine were preferred as neuromuscular blocker (92.9%) and antagonist (86.1%), respectively. Although most anesthesiologists recognized the detrimental effect of postoperative residual neuromuscular blockade (87.7%) and the importance of neuromuscular monitoring (76.3%), quantitative monitoring was available in only 51.2% of the hospitals. More than 75% of respondents still prefer to use clinical signs to evaluate the recovery from paralysis.
CONCLUSIONS
Changes in attitude and behaviors that mimic neuromuscular monitoring in Korea will be possible by regular and repeated publicity and education. Furthermore, greater distribution of neuromuscular monitoring devices and routine clinical use of these devices are also required.
Keyword
MeSH Terms
-
Anesthesiology
Cholinesterase Inhibitors
Delayed Emergence from Anesthesia
Education
Electronic Mail
Korea
Neuromuscular Blockade*
Neuromuscular Blocking Agents*
Neuromuscular Monitoring*
Neuromuscular Nondepolarizing Agents
Paralysis
Pyridostigmine Bromide
Specialization
Surveys and Questionnaires
Cholinesterase Inhibitors
Neuromuscular Blocking Agents
Neuromuscular Nondepolarizing Agents
Pyridostigmine Bromide
Figure
-
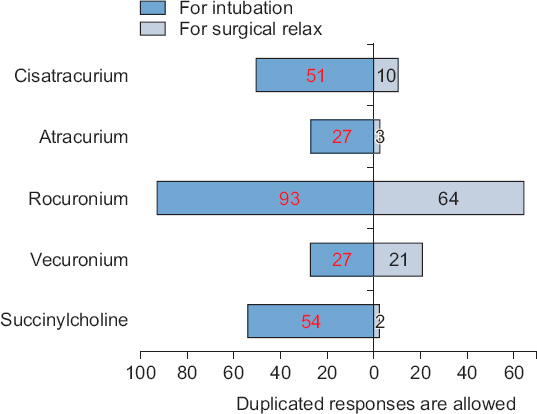
Fig. 1 Most often daily used neuromuscular blockers. This figure shows the data on the use of various neuromuscular blockers for tracheal intubation and surgical relaxation. Most of the respondents prefer to use a rocuronium for tracheal intubation and surgical relaxation. More than half of respondents still use succinylcholine for tracheal intubation.

Fig. 2 The availability of quantitative neuromuscular monitoring in the operating room (OR). In comparison of previous survey (Seo et al. [6]), the distribution rate decreased because the number of OR was increased rather than the supply of neuromuscular monitoring device over the years. TOF: train-of-four ratio.
Reference
-
1. Baillard C, Gehan G, Reboul-Marty J, Larmignat P, Samama CM, Cupa M. Residual curarization in the recovery room after vecuronium. Br J Anaesth. 2000; 84:394–5. DOI: 10.1093/oxfordjournals.bja.a013445. PMID: 10793602.2. Berg H, Roed J, Viby-Mogensen J, Mortensen CR, Engbaek J, Skovgaard LT, et al. Residual neuromuscular block is a risk factor for postoperative pulmonary complications. A prospective, randomised, and blinded study of postoperative pulmonary complications after atracurium, vecuronium and pancuronium. Acta Anaesthesiol Scand. 1997; 41:1095–103. DOI: 10.1111/j.1399-6576.1997.tb04851.x. PMID: 9366929.3. Bevan DR, Kahwaji R, Ansermino JM, Reimer E, Smith MF, O’Connor GA, et al. Residual block after mivacurium with or without edrophonium reversal in adults and children. Anesthesiology. 1996; 84:362–7. DOI: 10.1097/00000542-199602000-00014. PMID: 8602667.4. Debaene B, Plaud B, Dilly MP, Donati F. Residual paralysis in the PACU after a single intubating dose of nondepolarizing muscle relaxant with an intermediate duration of action. Anesthesiology. 2003; 98:1042–8. DOI: 10.1097/00000542-200305000-00004. PMID: 12717123.5. Brull SJ, Murphy GS. Residual neuromuscular block: lessons unlearned. Part II: methods to reduce the risk of residual weakness. Anesth Analg. 2010; 111:129–40. DOI: 10.1213/ANE.0b013e3181da8312. PMID: 20442261.6. Seo HJ, Lee YK, Lee SS, Kim KS, Yang HS. A survey of postoperative residual neuromuscular block and neuromuscular monitoring. Anesth Pain Med. 2010; 5:70–4.7. Eldawlatly A, El-Tahan MR. MMM-Anaesthesia Group Collaborators. A survey of the current use of neuromuscular blocking drugs among the Middle Eastern anesthesiologists. Saudi J Anaesth. 2013; 7:146–50. DOI: 10.4103/1658-354X.114063. PMID: 23956713. PMCID: PMC3737689.8. Naguib M, Kopman AF, Lien CA, Hunter JM, Lopez A, Brull SJ. A survey of current management of neuromuscular block in the United States and Europe. Anesth Analg. 2010; 111:110–9. DOI: 10.1213/ANE.0b013e3181c07428. PMID: 19910616.9. Viby-Mogensen J, Claudius C. Neuromuscular monitoring. Miller’s anaesthesia. 8th ed. Miller RD, Cohen NH, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Young WL, editors. Philadelphia: Elsevier;2015. p. 1604–21.10. Cronnelly R, Stanski DR, Miller RD, Sheiner LB. Pyridostigmine kinetics with and without renal function. Clin Pharmacol Ther. 1980; 28:78–81. DOI: 10.1038/clpt.1980.134. PMID: 6993086.11. Donati F, McCarroll SM, Antzaka C, McCready D, Bevan DR. Dose-response curves for edrophonium, neostigmine, and pyridostigmine after pancuronium and d-tubocurarine. Anesthesiology. 1987; 66:471–6. DOI: 10.1097/00000542-198704000-00004. PMID: 3565812.12. Fruergaard K, Viby-Mogensen J, Berg H, el-Mahdy AM. Tactile evaluation of the response to double burst stimulation decreases, but does not eliminate, the problem of postoperative residual paralysis. Acta Anaesthesiol Scand. 1998; 42:1168–74. DOI: 10.1111/j.1399-6576.1998.tb05271.x. PMID: 9834799.13. Murphy GS, Brull SJ. Residual neuromuscular block: lessons unlearned. Part I: definitions, incidence, and adverse physiologic effects of residual neuromuscular block. Anesth Analg. 2010; 111:120–8. DOI: 10.1213/ANE.0b013e3181da832d. PMID: 20442260.14. Ali HH, Utting JE, Gray TC. Quantitative assessment of residual antidepolarizing block. I. Br J Anaesth. 1971; 43:473–7. DOI: 10.1093/bja/43.5.473. PMID: 4254031.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- What anesthesiologists ask to know and should know about the neuromuscular monitoring: an updated review
- Current use of neuromuscular blocking agents and antagonists in Korea: a 2018 survey
- A survey of postoperative residual neuromuscular block and neuromuscular monitoring
- The latest trend in neuromuscular monitoring: return of the electromyography
- Neuromuscular blockade monitoring in pediatric patients
