Adverse Events During Perampanel Adjunctive Therapy in Intractable Epilepsy
- Affiliations
-
- 1Divison of Pediatric Neurology, Department of Pediatrics, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea. hdkimmd@yuhs.ac
- 2Department of Pediatrics, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2415044
- DOI: http://doi.org/10.3988/jcn.2018.14.3.296
Abstract
- BACKGROUND AND PURPOSE
Perampanel is the first α-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid (AMPA)-receptor antagonist developed to treat epilepsy. The effects of either rapid or slow dose titration on adverse events remain to be elucidated.
METHODS
Eighty-five patients received perampanel between March 2016 and August 2016. Patients were divided into two groups according to their dosing schedule: rapid dose titration (2-mg increments at intervals of 1 to 2 weeks) and slow dose titration (2-mg increments at intervals of at least 3 weeks). Seizure frequency and adverse events were analyzed over 3 months.
RESULTS
Adverse events were reported by 47 (58%) of the 81 patients analyzed, with 12 (15%) patients discontinuing perampanel due to adverse events. Common adverse events included dizziness (n=30, 37%), aggressive mood and behavior (n=19, 24%), gait disturbance (n=16, 20%), and sleep problems (n=10, 12.4%). The overall adverse events were similar in the slow-titration group (38 of 61 patients) and the rapid-titration group (8 of 20 patients, p=0.081). However, none of the 20 patients in the slow-titration group experienced gait disturbance, compared with 16 of the 61 patients in the rapid-titration group (p=0.009), while appetite change was experienced by 4 patients in the slow-titration group but only 1 in the rapid-titration group (p=0.003). No relationship was noted between adverse events and the maximum dose of perampanel (p=0.116). Sex differences were observed, with the response to perampanel being better and the rate of adverse events being higher in females (p=0.015 and p=0.046, respectively).
CONCLUSIONS
Slow titration of perampanel may reduce perampanel-related adverse events.
Keyword
MeSH Terms
Figure
-
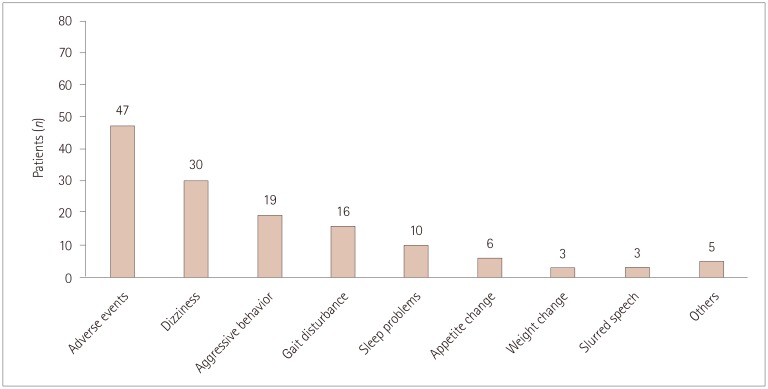
Fig. 1 Numbers of patients who experienced adverse events. The most-common adverse events were dizziness and somnolence, followed by aggressive mood and behavior. Other adverse events included excessive sputum production, drooling, dysphagia, nausea, memory impairment, and bizarre feeling.
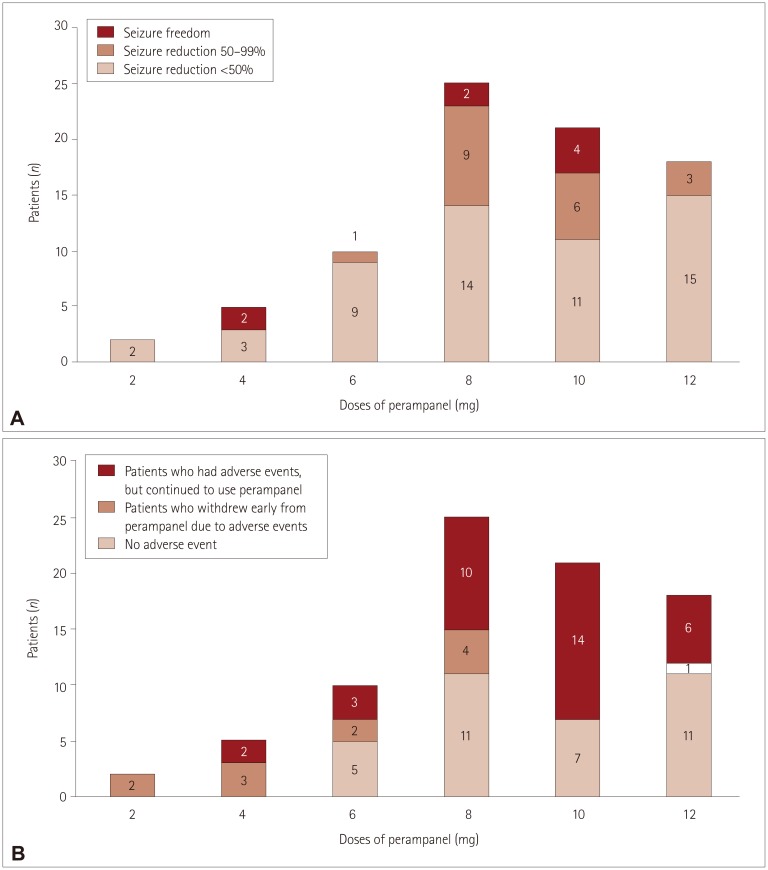
Fig. 2 Three-month seizure outcomes and occurrence of adverse events for different maximum doses of perampanel. A: The maximum doses were 2 and 4 mg in 7 patients. Two patients achieved seizure freedom when taking perampanel at the relatively low dose of 4 mg. The maximum doses were 6, 8, and 10 mg in more than two-thirds (56 of 81 patients) of patients. The rates of responders and seizure freedom were high for doses between 6 and 10 mg. The perampanel dose was increased to 12 mg when their seizures persisted, and no serious adverse events occurred. However, the rates of responders and seizure freedom were significantly low at a dose of 12 mg. B: Five patients stopped taking perampanel at low doses (e.g., 2 or 4 mg) due to adverse events. Only one patient stopped taking perampanel at 12 mg. Two patients who stopped at a dose of 2 mg experienced severe dizziness, and three patients who stopped at a dose of 4 mg reported experiencing multiple side effects including gait disturbance, dizziness, and aggressive behavior.
Reference
-
1. Rogawski MA. Revisiting AMPA receptors as an antiepileptic drug target. Epilepsy Curr. 2011; 11:56–63. PMID: 21686307.
Article2. French JA, Krauss GL, Biton V, Squillacote D, Yang H, Laurenza A, et al. Adjunctive perampanel for refractory partial-onset seizures: randomized phase III study 304. Neurology. 2012; 79:589–596. PMID: 22843280.
Article3. French JA, Krauss GL, Steinhoff BJ, Squillacote D, Yang H, Kumar D, et al. Evaluation of adjunctive perampanel in patients with refractory partial-onset seizures: results of randomized global phase III study 305. Epilepsia. 2013; 54:117–125. PMID: 22905857.
Article4. Krauss GL, Serratosa JM, Villanueva V, Endziniene M, Hong Z, French J, et al. Randomized phase III study 306: adjunctive perampanel for refractory partial-onset seizures. Neurology. 2012; 78:1408–1415. PMID: 22517103.
Article5. De Liso P, Vigevano F, Specchio N, De Palma L, Bonanni P, Osanni E, et al. Effectiveness and tolerability of perampanel in children and adolescents with refractory epilepsies: an Italian observational multicenter study. Epilepsy Res. 2016; 127:93–100. PMID: 27568598.6. Steinhoff BJ, Hamer H, Trinka E, Schulze-Bonhage A, Bien C, Mayer T, et al. A multicenter survey of clinical experiences with perampanel in real life in Germany and Austria. Epilepsy Res. 2014; 108:986–988. PMID: 24721197.
Article7. Steinhoff BJ, Bacher M, Bast T, Kornmeier R, Kurth C, Scholly J, et al. First clinical experiences with perampanel--the Kork experience in 74 patients. Epilepsia. 2014; 55(Suppl 1):16–18.
Article8. Shah E, Reuber M, Goulding P, Flynn C, Delanty N, Kemp S. Clinical experience with adjunctive perampanel in adult patients with uncontrolled epilepsy: a UK and Ireland multicentre study. Seizure. 2016; 34:1–5. PMID: 26615577.
Article9. Heyman E, Lahat E, Levin N, Epstein O, Lazinger M, Berkovitch M, et al. Tolerability and efficacy of perampanel in children with refractory epilepsy. Dev Med Child Neurol. 2017; 59:441–444. PMID: 27935018.
Article10. Biró A, Stephani U, Tarallo T, Bast T, Schlachter K, Fleger M, et al. Effectiveness and tolerability of perampanel in children and adolescents with refractory epilepsies: first experiences. Neuropediatrics. 2015; 46:110–116. PMID: 25730374.
Article11. Patsalos PN. The clinical pharmacology profile of the new antiepileptic drug perampanel: a novel noncompetitive AMPA receptor antagonist. Epilepsia. 2015; 56:12–27. PMID: 25495693.
Article12. Fisher RS. The new classification of seizures by the international league against epilepsy 2017. Curr Neurol Neurosci Rep. 2017; 17:48. PMID: 28425015.
Article13. Schalock RL, Borthwick-Duffy SA, Buntinx WHE, Coulter DL, Craig EM. Intellectual disability: definition, classification, and systems of supports. 11th ed. Washington, D.C.: American Association on Intellectual and Developmental Disabilities;2010.14. Trinka E, Steinhoff BJ, Nikanorova M, Brodie MJ. Perampanel for focal epilepsy: insights from early clinical experience. Acta Neurol Scand. 2016; 133:160–172. PMID: 26506904.
Article15. Gidal BE, Ferry J, Majid O, Hussein Z. Concentration-effect relationships with perampanel in patients with pharmacoresistant partial-onset seizures. Epilepsia. 2013; 54:1490–1497. PMID: 23772853.
Article16. Franconi F, Brunelleschi S, Steardo L, Cuomo V. Gender differences in drug responses. Pharmacol Res. 2007; 55:81–95. PMID: 17129734.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy and Tolerability of Low-Dose Perampanel in Patients with Childhood-Onset Intractable Epilepsy
- Real-Life Effectiveness and Tolerability of Perampanel in Pediatric Patients Aged 4 Years or Older with Epilepsy: A Korean National Multicenter Study
- New antiepileptic drugs: usage, adverse effects, and interactions
- Efficacy of levetiracetam in refractory childhood epilepsy
- A meta-analysis: efficacy and safety of anti-epileptic drugs prescribed in Korea as monotherapy and adjunctive treatment for patients with focal epilepsy
