Acute Gastritis and Splenic Infarction Caused by Epstein-Barr Virus
- Affiliations
-
- 1Department of Pediatrics, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. hl.jung@samsung.com
- 2Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2409367
- DOI: http://doi.org/10.5223/pghn.2018.21.2.147
Abstract
- Epstein-Barr virus (EBV) infection can be presented with various clinical manifestations and different levels of severity when infected. Infectious mononucleosis, which is most commonly caused by EBV infection in children and adolescents, is a clinical syndrome characterized by fatigue, malaise, fever, sore throat, and generalized lymphadenopathy. But rarely, patients with infectious mononucleosis may present with gastrointestinal symptoms and complicated by gastritis, splenic infarction, and splenic rupture. We encountered a 16-year-old girl who presented with fever, fatigue, and epigastric pain. Splenic infarction and EBV-associated gastritis were diagnosed by using esophagogastroduodenoscopy and abdominal computed tomography. Endoscopy revealed a generalized hyperemic nodular lesion in the stomach, and the biopsy findings were chronic gastritis with erosion and positive in situ hybridization for EBV. As splenic infarction and acute gastritis are rare in infectious mononucleosis and are prone to be overlooked, we must consider these complications when an infectious mononucleosis patient presents with gastrointestinal symptom.
MeSH Terms
Figure
-

Fig. 1 Abdominal and pelvis computed tomography (CT) showed (A) hepatosplenomegaly and 2×1.6 cm, sized low attenuated lesion (white arrow), which that was consistent with splenic infarction; and (B) multiple slightly enlarged lymph nodes around aorta and mesentery (white arrows). Follow-up abdominal ultrasonography on the fifth hospital day showed (C) no sonographic evidence of splenic infarction or other focal lesion of the spleen.
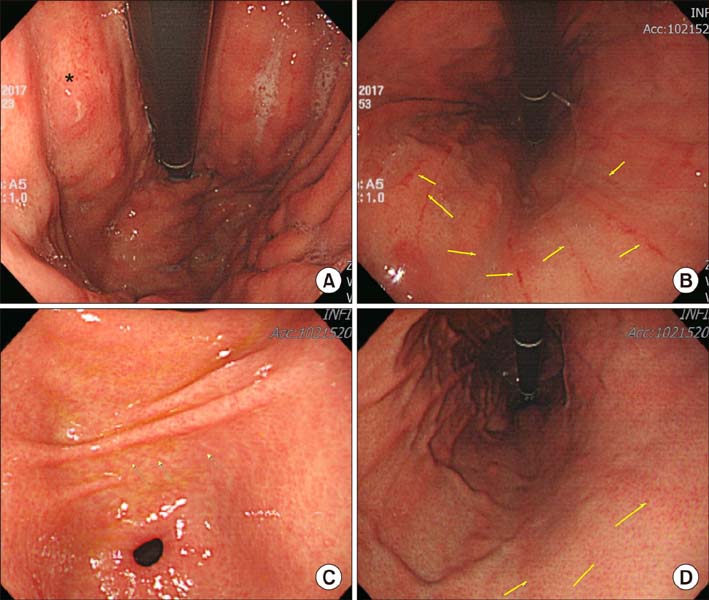
Fig. 2 Characteristics of the patient's esophagogastroduodenoscopy (EGD) image Endoscopic image showing (A) hyperemic nodular lesion (asterisk) and (B) linear erosions (arrows). Five months after discharge, follow up EGD revealed (C, D) linear red streak detected on the body large curvature side (arrows).
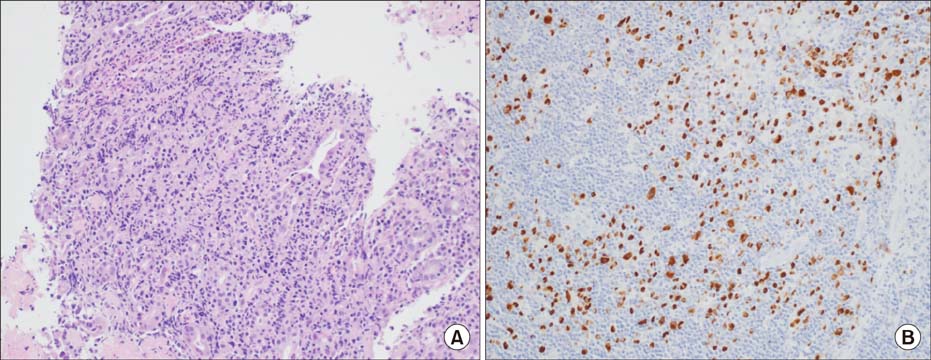
Fig. 3 Microscopic findings. (A) There is diffuse atypical lymphocytes proliferation in the lamina propria (H&E, ×200). (B) It shows positive for Epstein-Barr virus-encoded DNA staining (in situ hybridization method, ×200).
Reference
-
1. Luzuriaga K, Sullivan JL. Epstein-Barr virus. In : Richman DD, Whitley RJ, Hayden FG, editors. Clinical virology. 3rd ed. Washington, DC: ASM Press;2009. p. 521–536.2. Evans AS, Niederman JC, Cenabre LC, West B, Richards VA. A prospective evaluation of heterophile and Epstein-Barr virus-specific IgM antibody tests in clinical and subclinical infectious mononucleosis: specificity and sensitivity of the tests and persistence of antibody. J Infect Dis. 1975; 132:546–554.
Article3. Kim JM, Song CW, Song KS, Kim JY. Acute gastritis associated with Epstein-Barr virus infection in a child. Korean J Pediatr. 2016; 59:Suppl 1. S68–S71.
Article4. Gang MH, Kim JY. Splenic infarction in a child with primary Epstein-Barr virus infection. Pediatr Int. 2013; 55:e126–e128.
Article5. Luzuriaga K, Sullivan JL. Infectious mononucleosis. N Engl J Med. 2010; 362:1993–2000.
Article6. Tselis A, Duman R, Storch GA, Lisak RP. Epstein-Barr virus encephalomyelitis diagnosed by polymerase chain reaction: detection of the genome in the CSF. Neurology. 1997; 48:1351–1355.
Article7. Haller A, von Segesser L, Baumann PC, Krause M. Severe respiratory insufficiency complicating Epstein-Barr virus infection: case report and review. Clin Infect Dis. 1995; 21:206–209.
Article8. Jenson HB. Epstein-Barr virus. In : Kliegman R, Stanton B, St. Geme J, Schor N, editors. Nelson textbook of pediatrics. 20th ed. Philadelphia: Elsevier;2015. p. 1586–1590.9. Tynell E, Aurelius E, Brandell A, Julander I, Wood M, Yao QY, et al. Acyclovir and prednisolone treatment of acute infectious mononucleosis: a multicenter, double-blind, placebo-controlled study. J Infect Dis. 1996; 174:324–331.
Article10. Hisamatsu A, Nagai T, Okawara H, Nakashima H, Tasaki T, Nakagawa Y, et al. Gastritis associated with Epstein-Barr virus infection. Intern Med. 2010; 49:2101–2105.
Article11. Zhang Y, Molot R. Severe gastritis secondary to Epstein-Barr viral infection. Unusual presentation of infectious mononucleosis and associated diffuse lymphoid hyperplasia in gastric mucosa. Arch Pathol Lab Med. 2003; 127:478–480.12. Kitayama Y, Honda S, Sugimura H. Epstein-Barr virus-related gastric pseudolymphoma in infectious mononucleosis. Gastrointest Endosc. 2000; 52:290–291.
Article13. Jung JK, Chung JP, Kim KC, Park HJ, Lee KS, Chon CY, et al. A case of Epstein-Barr virus-associated primary gastric T-cell lymphoma with rapidly progressive endoscopic features and clinical course. Korean J Gastrointest Endosc. 1999; 19:438–442.14. Ueo T, Kashima K, Daa T, Kondo Y, Yokoyama S. Coexistence of Epstein-Barr virus-associated gastric carcinoma with malignant lymphoma: report of two cases. Virchows Arch. 2006; 449:215–219.
Article15. Thorley-Lawson DA, Gross A. Persistence of the Epstein-Barr virus and the origins of associated lymphomas. N Engl J Med. 2004; 350:1328–1337.
Article16. Jaroch MT, Broughan TA, Hermann RE. The natural history of splenic infarction. Surgery. 1986; 100:743–750.17. Antopolsky M, Hiller N, Salameh S, Goldshtein B, Stalnikowicz R. Splenic infarction: 10 years of experience. Am J Emerg Med. 2009; 27:262–265.
Article18. García-Carrasco M, Galarza-Maldonado C, Mendoza-Pinto C, Escarcega RO, Cervera R. Infections and the antiphospholipid syndrome. Clin Rev Allergy Immunol. 2009; 36:104–108.
Article19. Maier W. Computed tomography in the diagnosis of splenic infarction. Eur J Radiol. 1982; 2:202–204.20. Asgari MM, Begos DG. Spontaneous splenic rupture in infectious mononucleosis: a review. Yale J Biol Med. 1997; 70:175–182.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute gastritis associated with Epstein-Barr virus infection in a child
- A Case of Epstein-Barr Virus-Associated Hemophagocytic Syndrome Demonstrated by In Situ Hybridization
- A Case of Epstein-Barr Virus-Positive Diffuse Large B-Cell Lymphoma Occurring in Thyroid Gland
- A Case of Epstein-Barr Virus-Related Dacryoadenitis
- A Case of Epstein-Barr Virus-Associated Hemophagocytic Syndrome with Ascites
