High-Sensitivity C-Reactive Protein Can Reflect Small Airway Obstruction in Childhood Asthma
- Affiliations
-
- 1Department of Pediatrics, Severance Hospital, Institute of Allergy, Brain Korea 21 PLUS Project for Medical Science, Yonsei University College of Medicine, Seoul, Korea. yhkim@yuhs.ac
- KMID: 2374090
- DOI: http://doi.org/10.3349/ymj.2016.57.3.690
Abstract
- PURPOSE
High-sensitivity assays enabled the identification of C-reactive protein (hs-CRP) at levels that were previously undetectable. We aimed to determine if hs-CRP could reflect airway inflammation in children, by comparing hs-CRP with spirometry and impulse oscillometry (IOS) parameters and symptomatic severities.
MATERIALS AND METHODS
A total of 276 asthmatic children who visited Severance Children's Hospital from 2012-2014 were enrolled. Serum hs-CRP and pulmonary function tests were performed on the same day. Patients were divided into hs-CRP positive and negative groups (cut-off value, 3.0 mg/L).
RESULTS
Of the 276 asthmatic children [median age 7.5 (5.9/10.1) years, 171 boys (62%)], 39 were hs-CRP positive and 237 were negative. Regarding spirometry parameters, we observed significant differences in maximum mid-expiratory flow, % predicted (FEF25-75) (p=0.010) between hs-CRP positive and negative groups, and a negative correlation between FEF25-75 and hs-CRP. There were significant differences in the reactance area (AX) (p=0.046), difference between resistance at 5 Hz and 20 Hz (R5-R20) (p=0.027), resistance at 5 Hz, % predicted (R5) (p=0.027), and reactance at 5 Hz, % predicted (X5) (p=0.041) between hs-CRP positive and negative groups. There were significant positive correlations between hs-CRP and R5 (r=0.163, p=0.008), and X5 (r=0.164, p=0.007). Spirometry and IOS parameters had more relevance in patients with higher blood neutrophil levels in comparison to hs-CRP.
CONCLUSION
Hs-CRP showed significant correlation with FEF25-75, R5, and X5. It can reflect small airway obstruction in childhood asthma, and it is more prominent in neutrophil dominant inflammation.
MeSH Terms
-
Airway Obstruction/*diagnosis/etiology
Asthma/*diagnosis/physiopathology
C-Reactive Protein/*analysis
Child
Child, Preschool
Female
Forced Expiratory Volume
Humans
Inflammation/*etiology
Male
Neutrophils/metabolism
Oscillometry/*methods
Respiratory Function Tests/*methods
Respiratory System
Sensitivity and Specificity
*Spirometry
C-Reactive Protein
Figure
-
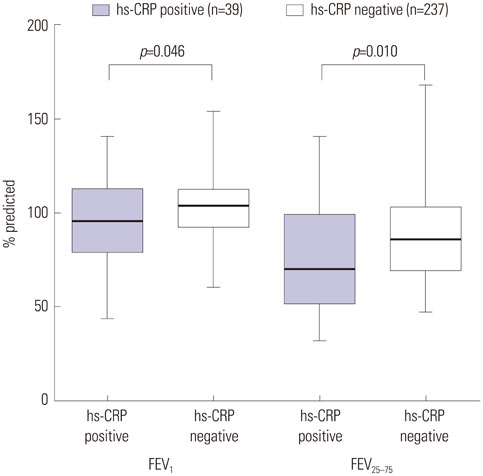
Fig. 1 Comparisons of forced expiratory volume in 1 second, % predicted (FEV1) and maximum midexpiratory flow, % predicted (FEF25–75) between high-sensitivity C-reactive protein (hs-CRP) positive and negative groups. FEV1 (p=0.046) and FEF25–75 (p=0.010) were significantly lower in the hs-CRP positive group than in the negative group.
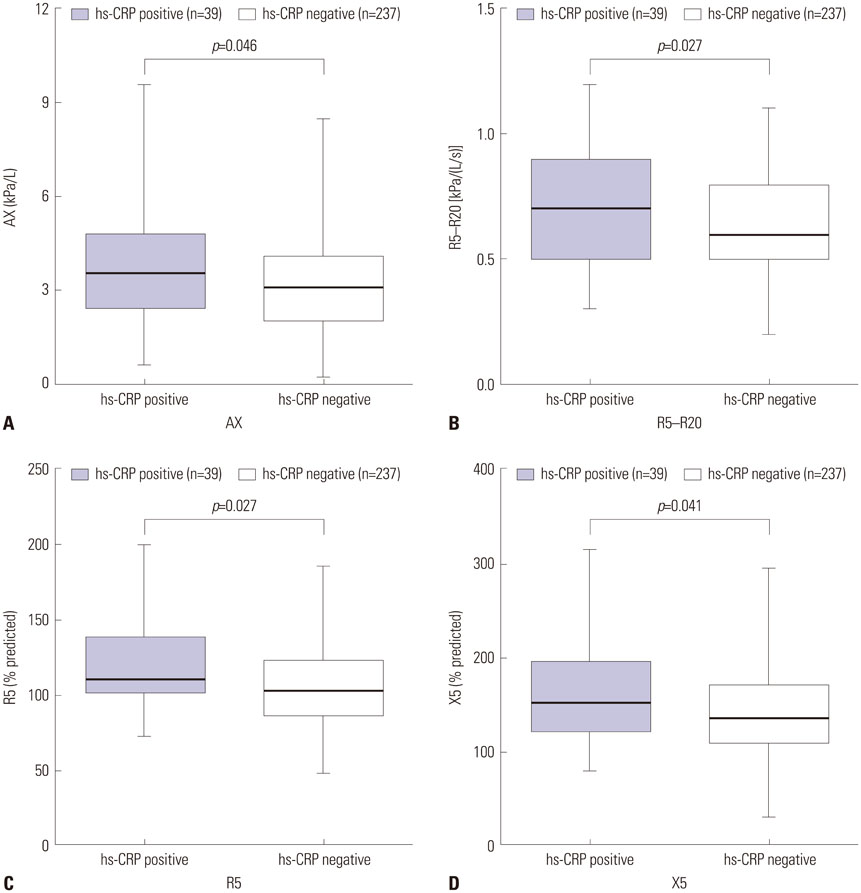
Fig. 2 Comparisons of impulse oscillometry (IOS) parameters between high-sensitivity (hs-CRP) positive and negative groups. (A) Reactance area (AX) was significantly higher in the hs-CRP positive group than in the negative group (p=0.046). (B) Difference between resistance at 5 Hz and 20 Hz (R5–R20) was significantly higher in the hs-CRP positive group than in the negative group (p=0.027). (C) Resistance at 5 Hz, % predicted (R5) was significantly higher in the hs-CRP positive group than in the negative group (p=0.027). (D) Reactance at 5 Hz, % predicted (X5) was significantly higher in the hs-CRP positive group than in the negative group (p=0.041).
Reference
-
1. van de Kant KD, Klaassen EM, Jöbsis Q, Nijhuis AJ, van Schayck OC, Dompeling E. Early diagnosis of asthma in young children by using non-invasive biomarkers of airway inflammation and early lung function measurements: study protocol of a case-control study. BMC Public Health. 2009; 9:210.
Article2. Deraz TE, Kamel TB, El-Kerdany TA, El-Ghazoly HM. High-sensitivity C reactive protein as a biomarker for grading of childhood asthma in relation to clinical classification, induced sputum cellularity, and spirometry. Pediatr Pulmonol. 2012; 47:220–225.
Article3. Busse WW, Lemanske RF Jr. Asthma. N Engl J Med. 2001; 344:350–362.
Article4. Jousilahti P, Salomaa V, Hakala K, Rasi V, Vahtera E, Palosuo T. The association of sensitive systemic inflammation markers with bronchial asthma. Ann Allergy Asthma Immunol. 2002; 89:381–385.
Article5. Hoshino M, Ohtawa J, Akitsu K. Increased C-reactive protein is associated with airway wall thickness in steroid-naive asthma. Ann Allergy Asthma Immunol. 2014; 113:37–41.
Article6. Ramirez D, Patel P, Casillas A, Cotelingam J, Boggs P, Bahna SL. Assessment of high-sensitivity C-reactive protein as a marker of airway inflammation in asthma. Ann Allergy Asthma Immunol. 2010; 104:485–489.
Article7. Kilic H, Karalezli A, Hasanoglu HC, Erel O, Ates C. The relationship between hs-CRP and asthma control test in asthmatic patients. Allergol Immunopathol (Madr). 2012; 40:362–367.
Article8. Ridker PM. High-sensitivity C-reactive protein: potential adjunct for global risk assessment in the primary prevention of cardiovascular disease. Circulation. 2001; 103:1813–1818.
Article9. Takemura M, Matsumoto H, Niimi A, Ueda T, Matsuoka H, Yamaguchi M, et al. High sensitivity C-reactive protein in asthma. Eur Respir J. 2006; 27:908–912.
Article10. Shimoda T, Obase Y, Kishikawa R, Iwanaga T. Serum high-sensitivity C-reactive protein can be an airway inflammation predictor in bronchial asthma. Allergy Asthma Proc. 2015; 36:e23–e28.
Article11. Rifai N, Tracy RP, Ridker PM. Clinical efficacy of an automated highsensitivity C-reactive protein assay. Clin Chem. 1999; 45:2136–2141.
Article12. Sahoo RC, Acharya PR, Noushad TH, Anand R, Acharya VK, Sahu KR. A study of high-sensitivity C-reactive protein in bronchial asthma. Indian J Chest Dis Allied Sci. 2009; 51:213–216.13. Zietkowski Z, Tomasiak-Lozowska MM, Skiepko R, Mroczko B, Szmitkowski M, Bodzenta-Lukaszyk A. High-sensitivity C-reactive protein in the exhaled breath condensate and serum in stable and unstable asthma. Respir Med. 2009; 103:379–385.
Article14. Sävykoski T, Harju T, Paldanius M, Kuitunen H, Bloigu A, Wahlström E, et al. Chlamydia pneumoniae infection and inflammation in adults with asthma. Respiration. 2004; 71:120–125.
Article15. Kony S, Zureik M, Driss F, Neukirch C, Leynaert B, Neukirch F. Association of bronchial hyperresponsiveness and lung function with C-reactive protein (CRP): a population based study. Thorax. 2004; 59:892–896.
Article16. Fujita M, Ueki S, Ito W, Chiba T, Takeda M, Saito N, et al. C-reactive protein levels in the serum of asthmatic patients. Ann Allergy Asthma Immunol. 2007; 99:48–53.
Article17. Shaaban R, Kony S, Driss F, Leynaert B, Soussan D, Pin I, et al. Change in C-reactive protein levels and FEV1 decline: a longitudinal population-based study. Respir Med. 2006; 100:2112–2120.
Article18. Olafsdottir IS, Gislason T, Thjodleifsson B, Olafsson I, Gislason D, Jögi R, et al. C reactive protein levels are increased in non-allergic but not allergic asthma: a multicentre epidemiological study. Thorax. 2005; 60:451–454.
Article19. Navratil M, Plavec D, Dodig S, Jelcic Z, Nogalo B, Erceg D, et al. Markers of systemic and lung inflammation in childhood asthma. J Asthma. 2009; 46:822–828.
Article20. Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, et al. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 2000; 161:309–329.21. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003; 107:499–511.22. Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010; 122:e584–e636.23. Goldman MD. Clinical application of forced oscillation. Pulm Pharmacol Ther. 2001; 14:341–350.
Article24. Komarow HD, Myles IA, Uzzaman A, Metcalfe DD. Impulse oscillometry in the evaluation of diseases of the airways in children. Ann Allergy Asthma Immunol. 2011; 106:191–199.
Article25. Pepys MB. C-reactive protein fifty years on. Lancet. 1981; 1:653–657.
Article26. Pepys MB, Baltz ML. Acute phase proteins with special reference to C-reactive protein and related proteins (pentaxins) and serum amyloid A protein. Adv Immunol. 1983; 34:141–212.
Article27. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999; 340:448–454.
Article28. Wouters EF, Reynaert NL, Dentener MA, Vernooy JH. Systemic and local inflammation in asthma and chronic obstructive pulmonary disease: is there a connection? Proc Am Thorac Soc. 2009; 6:638–647.
Article29. Wilkinson TM, Donaldson GC, Johnston SL, Openshaw PJ, Wedzicha JA. Respiratory syncytial virus, airway inflammation, and FEV1 decline in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2006; 173:871–876.
Article30. Maclay JD, McAllister DA, Macnee W. Cardiovascular risk in chronic obstructive pulmonary disease. Respirology. 2007; 12:634–641.
Article31. Livnat G, Yoseph RB, Nir V, Hakim F, Yigla M, Bentur L. Evaluation of high-sensitivity serum CRP levels compared to markers of airway inflammation and allergy as predictors of methacholine bronchial hyper-responsiveness in children. Lung. 2015; 193:39–45.
Article32. Weiss ST, Tosteson TD, Segal MR, Tager IB, Redline S, Speizer FE. Effects of asthma on pulmonary function in children. A longitudinal population-based study. Am Rev Respir Dis. 1992; 145:58–64.
Article33. Rao DR, Gaffin JM, Baxi SN, Sheehan WJ, Hoffman EB, Phipatanakul W. The utility of forced expiratory flow between 25% and 75% of vital capacity in predicting childhood asthma morbidity and severity. J Asthma. 2012; 49:586–592.
Article34. Beydon N, Davis SD, Lombardi E, Allen JL, Arets HG, Aurora P, et al. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med. 2007; 175:1304–1345.
Article35. Wood LG, Baines KJ, Fu J, Scott HA, Gibson PG. The neutrophilic inflammatory phenotype is associated with systemic inflammation in asthma. Chest. 2012; 142:86–93.
Article36. Halvani A, Tahghighi F, Nadooshan HH. Evaluation of correlation between airway and serum inflammatory markers in asthmatic patients. Lung India. 2012; 29:143–146.
Article37. Butland BK, Strachan DP, Rudnicka AR. C-reactive protein, obesity, atopy and asthma symptoms in middle-aged adults. Eur Respir J. 2008; 32:77–84.
Article38. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009; 33:1165–1185.
Article39. Fu JJ, Baines KJ, Wood LG, Gibson PG. Systemic inflammation is associated with differential gene expression and airway neutrophilia in asthma. OMICS. 2013; 17:187–199.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bronchial Structural Changes in Childhood Asthma
- Viral Infections and the Inception and Exacerbation of Asthma
- Phenotypes and endotypes of severe asthma in children
- Evolution of Asthma Concept and Effect of Current Asthma Management Guidelines
- Systemic Inflammation in Older Adults With Asthma-COPD Overlap Syndrome
