Endocrinol Metab.
2016 Sep;31(3):424-432. 10.3803/EnM.2016.31.3.424.
Prognostic Factors in Patients Hospitalized with Diabetic Ketoacidosis
- Affiliations
-
- 1Department of Medicine, King George's Medical College, Lucknow, India. manish07gutch@gmail.com
- 2Department of Obstetrics and Gynecology, King George's Medical College, Lucknow, India.
- 3Department of Radiodiagnosis, King George's Medical College, Lucknow, India.
- 4Department of Pulmonary Medicine, King George's Medical College, Lucknow, India.
- 5Department of Physical Medicine and Rehabilitation, King George's Medical College, Lucknow, India.
- KMID: 2352982
- DOI: http://doi.org/10.3803/EnM.2016.31.3.424
Abstract
- BACKGROUND
Diabetic ketoacidosis (DKA) is characterized by a biochemical triad of hyperglycemia, acidosis, and ketonemia. This condition is life-threatening despite improvements in diabetic care. The purpose of this study was to evaluate the clinical and biochemical prognostic markers of DKA. We assessed correlations in prognostic markers with DKA-associated morbidity and mortality.
METHODS
Two hundred and seventy patients that were hospitalized with DKA over a period of 2 years were evaluated clinically and by laboratory tests. Serial assays of serum electrolytes, glucose, and blood pH were performed, and clinical outcome was noted as either discharged to home or death.
RESULTS
The analysis indicated that significant predictors included sex, history of type 1 diabetes mellitus or type 2 diabetes mellitus, systolic blood pressure, diastolic blood pressure, total leukocyte count, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, blood urea nitrogen, serum creatinine, serum magnesium, serum phosphate, serum osmolality, serum glutamic oxaloacetic transaminases, serum glutamic pyruvic transaminases, serum albumin, which were further regressed and subjected to multivariate logistic regression (MLR) analysis. The MLR analysis indicated that males were 7.93 times more likely to have favorable outcome compared with female patients (odds ratio, 7.93; 95% confidence interval, 3.99 to 13.51), while decreases in mean APACHE II score (14.83) and serum phosphate (4.38) at presentation may lead to 2.86- and 2.71-fold better outcomes, respectively, compared with higher levels (APACHE II score, 25.00; serum phosphate, 6.04).
CONCLUSION
Sex, baseline biochemical parameters such as APACHE II score, and phosphate level were important predictors of the DKA-associated mortality.
MeSH Terms
-
Acidosis
APACHE
Blood Pressure
Blood Urea Nitrogen
Creatinine
Diabetes Mellitus, Type 1
Diabetes Mellitus, Type 2
Diabetic Ketoacidosis*
Electrolytes
Female
Glucose
Humans
Hydrogen-Ion Concentration
Hyperglycemia
Hyperglycemic Hyperosmolar Nonketotic Coma
Ketosis
Leukocyte Count
Logistic Models
Magnesium
Male
Mortality
Osmolar Concentration
Serum Albumin
Transaminases
Creatinine
Electrolytes
Glucose
Magnesium
Serum Albumin
Transaminases
Figure
-
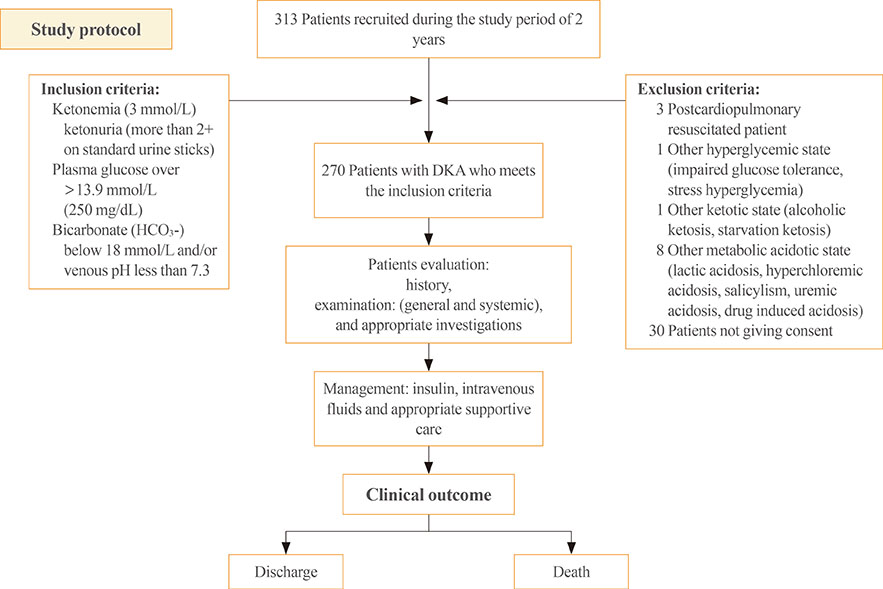
Fig. 1 Study protocol. DKA, diabetic ketoacidosis.
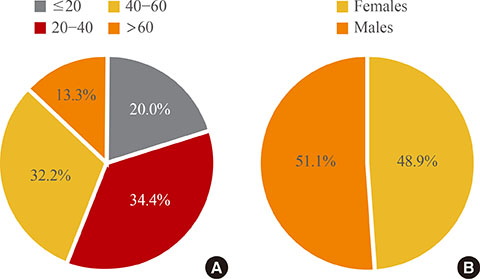
Fig. 2 (A) Age and (B) sex distributions.
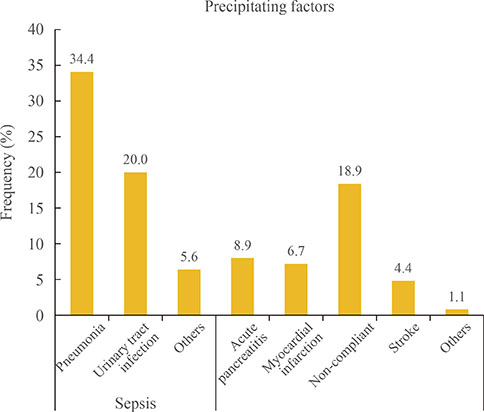
Fig. 3 Precipitating factors.
Reference
-
1. Kearney T, Dang C. Diabetic and endocrine emergencies. Postgrad Med J. 2007; 83:79–86.2. Delaney MF, Zisman A, Kettyle WM. Diabetic ketoacidosis and hyperglycemic hyperosmolar nonketotic syndrome. Endocrinol Metab Clin North Am. 2000; 29:683–705.3. Chu CH, Lee JK, Lam HC, Lu CC. Prognostic factors of hyperglycemic hyperosmolar nonketotic state. Chang Gung Med J. 2001; 24:345–351.4. National Diabetes Data Group. National Institute of Diabetes and Digestive and Kidney Diseases. Chapter 13, Acute metabolic complications in diabetes. Diabetes in America. 2nd ed. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases;1995. p. 283–292.5. Kitabchi AE, Umpierrez GE, Murphy MB, Kreisberg RA. Hyperglycemic crises in adult patients with diabetes: a consensus statement from the American Diabetes Association. Diabetes Care. 2006; 29:2739–2748.6. Umpierrez GE, Smiley D, Kitabchi AE. Narrative review: ketosis-prone type 2 diabetes mellitus. Ann Intern Med. 2006; 144:350–357.7. Balasubramanyam A, Zern JW, Hyman DJ, Pavlik V. New profiles of diabetic ketoacidosis: type 1 vs type 2 diabetes and the effect of ethnicity. Arch Intern Med. 1999; 159:2317–2322.8. Singh RK, Perros P, Frier BM. Hospital management of diabetic ketoacidosis: are clinical guidelines implemented effectively? Diabet Med. 1997; 14:482–486.9. Sola E, Garzon S, Garcia-Torres S, Cubells P, Morillas C, Hernandez-Mijares A. Management of diabetic ketoacidosis in a teaching hospital. Acta Diabetol. 2006; 43:127–130.10. Ellemann K, Soerensen JN, Pedersen L, Edsberg B, Andersen OO. Epidemiology and treatment of diabetic ketoacidosis in a community population. Diabetes Care. 1984; 7:528–532.11. Gutch M, Razi SM, Kumar S, Gupta KK. Diabetes mellitus: trends in northern India. Indian J Endocrinol Metab. 2014; 18:731–734.12. Oschatz E, Mullner M, Herkner H, Laggner AN. Multiple organ failure and prognosis in adult patients with diabetic ketoacidosis. Wien Klin Wochenschr. 1999; 111:590–595.13. Umpierrez GE, Murphy MB, Kitabchi AE. Diabetic ketoacidosis and hyperglycemic hyperosmolar syndrome. Diabetes Spectr. 2002; 15:28–36.14. Randall L, Begovic J, Hudson M, Smiley D, Peng L, Pitre N, et al. Recurrent diabetic ketoacidosis in inner-city minority patients: behavioral, socioeconomic, and psychosocial factors. Diabetes Care. 2011; 34:1891–1896.15. Barski L, Nevzorov R, Harman-Boehm I, Jotkowitz A, Rabaev E, Zektser M, et al. Comparison of diabetic ketoacidosis in patients with type-1 and type-2 diabetes mellitus. Am J Med Sci. 2013; 345:326–330.16. Bassyouni A, El Ebrashy I, El Hefnawy H. Epidemiology of diabetic ketoacidosis in National Institute of Diabetes and Endocrinology. Endocr Abstr. 2012; 29:659.17. Otieno CF, Kayima JK, Mbugua PK, Amayo AA, Mcligeyo SO. Prognostic factors in patients hospitalised with diabetic ketoacidosis at Kenyatta National Hospital, Nairobi. East Afr Med J. 2010; 87:66–73.18. Slovis CM, Mork VG, Slovis RJ, Bain RP. Diabetic ketoacidosis and infection: leukocyte count and differential as early predictors of serious infection. Am J Emerg Med. 1987; 5:1–5.19. Razavi Nematollahi L, Kitabchi AE, Stentz FB, Wan JY, Larijani BA, Tehrani MM, et al. Proinflammatory cytokines in response to insulin-induced hypoglycemic stress in healthy subjects. Metabolism. 2009; 58:443–448.20. Kebler R, McDonald FD, Cadnapaphornchai P. Dynamic changes in serum phosphorus levels in diabetic ketoacidosis. Am J Med. 1985; 79:571–576.21. Shen T, Braude S. Changes in serum phosphate during treatment of diabetic ketoacidosis: predictive significance of severity of acidosis on presentation. Intern Med J. 2012; 42:1347–1350.22. Jayashree M, Singhi S. Diabetic ketoacidosis: predictors of outcome in a pediatric intensive care unit of a developing country. Pediatr Crit Care Med. 2004; 5:427–433.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Insulin Autoimmune Syndrome with Diabetic Ketoacidosis
- New Onset Diabetic Ketoacidosis Associated with Quetiapine
- A case of hyperthyroidism presented as diabetic ketoacidosis
- A Case of Acromegaly Presenting with Diabetic Ketoacidosis
- Diabetic Ketoacidosis Associated with Emphysematous Gastritis: A Case Report
