Prediction of Brobchodilator Response by Using FEF25~75% in Adult Patient with a Normal Spirometry Result
- Affiliations
-
- 1Division of Pulmology and Allergy, Department of Internal Medicine, Eulji Medical Center, Eulji University School of Medicine, Korea. hoonakr@eulji.ac.kr
Abstract
- BACKGROUND
When patients with chronic respiratory symptoms have a normal spirometry result, it is not always easy to consider bronchial asthma as the preferential diagnosis. Forced expiratory flow between 25% and 75% of vital capacity (FEF(25~75%)) is known as a useful diagnostic value of small airway diseases. However, it is not commonly used, because of its high individual variability. We evaluated the pattern of bronchodilator responsiveness (BDR) and the correlation between FEF25~75% and BDR in patients with suspicious asthma and normal spirometry.
METHODS
Among patients with suspicious bronchial asthma, 440 adult patients with a normal spirometry result (forced expiratory volume in one second [FEV1]/forced vital capacity [FVC] > or =70% & FEV1% predicted > or =80%) were enrolled. We divided this group into a positive BDR group (n=43) and negative BDR group (n=397), based on the result of BDR. A comparison was carried out of spirometric parameters with % change of FEV1 after bronchodilator (DeltaFEV1%).
RESULTS
Among the 440 patients with normal spirometry, FEF(25~75%)% predicted were negatively correlated with DeltaFEV1% (r=-0.22, p<0.01), and BDR was positive in 43 patients (9.78%). The means of FEF(25~75%)% predicted were 64.0+/-14.5% in the BDR (+) group and 72.9+/-20.8% in the BDR (-) group (p<0.01). The negative correlation between FEF(25~75%)% predicted and DeltaFEV1% was stronger in the BDR (+) group (r=-0.38, p=0.01) than in the BDR (-) group (r=-0.17, p<0.01). In the ROC curve analysis, FEF(25~75%) at 75% of predicted value had 88.3% sensitivity and 40.3% specificity for detecting a positive BDR.
CONCLUSION
BDR (+) was not rare in patients with suspicious asthma and normal spirometry. In these patients, FEF(25~75%)% predicted was well correlated with BDR.
Keyword
MeSH Terms
Figure
-
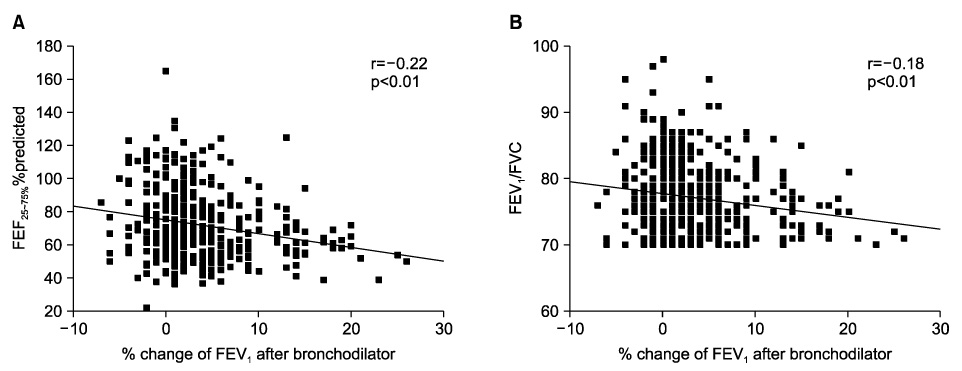
Figure 1 (A) Correlation between % change of FEV1 after bronchodilator (ΔFEV1%) and FEF25~75%% predicted value in total patients with suspicious asthma and normal spirometry (r=-0.22, p<0.01) and (B) correlation between ΔFEV1% and FEV1/FVC in total patients with suspicious asthma and normal spirometry (r=-0.18, p<0.01). Among 43 patients with positive bronchodilator response (ΔFEV1% ≥12%), the number of patients with FEF25~75% more than 80% predicted value is four and that of patients with FEV1/FVC more than 80% is seven. FVC: forced vital capacity; FEV1: forced expiratory volume in one second; FEF25~75%: forced expiratory flow between 25 and 75% of vital capacity.

Figure 2 (A) ROC curve of FEF25~75%% predicted for bronchodilator responsiveness as a change of more than 12% and 200 mL in FEV1 (p<0.01) and (B) ROC curve of FEV1/FVC for bronchodilator responsiveness as a change of more than 12% and 200 mL in FEV1 (p=0.03). The inflection value for FEF25~75% is at 75% of predicted value and that for the FEV1/FVC ratio is at 79% of predicted value. ROC: receiver operating characteristic; AUC: area under curve; FEF25~75%: forced expiratory flow between 25 and 75% of vital capacity; FVC: forced vital capacity; FEV1: forced expiratory volume in one second.
Reference
-
1. Kaplan AG, Balter MS, Bell AD, Kim H, McIvor RA. Diagnosis of asthma in adults. CMAJ. 2009. 181:E210–E220.2. Hamid Q, Song Y, Kotsimbos TC, Minshall E, Bai TR, Hegele RG, et al. Inflammation of small airways in asthma. J Allergy Clin Immunol. 1997. 100:44–51.3. Alberts WM, Ferris MC, Brooks SM, Goldman AL. The FEF25-75% and the clinical diagnosis of asthma. Ann Allergy. 1994. 73:221–225.4. Lougheed MD, Lemière C, Dell SD, Ducharme FM, Fitzgerald JM, Leigh R, et al. Canadian Thoracic Society Asthma Management Continuum--2010 Consensus summary for children six years of age and over, and adults. Can Respir J. 2010. 17:15–24.5. Choi BW, Yoo KH, Jeong JW, Yoon HJ, Kim SH, Park YM, et al. Easy diagnosis of asthma: computer-assisted, symptom-based diagnosis. J Korean Med Sci. 2007. 22:832–838.6. McFadden ER Jr, Linden DA. A reduction in maximum mid-expiratory flow rate. A spirographic manifestation of small airway disease. Am J Med. 1972. 52:725–737.7. Jung SY, Lee ES, Lee YH, Moon HK. Evaluation of the severity in patients with bronchial asthma using FEF25-75%. J Korean Pediatr Soc. 2001. 44:916–921.8. Rhee KH, Kim JK, Kim JH, Lim DH, Son BK. Usefulness of FEF25-75% in methacholine bronchial provocation test in children with asthma. Pediatr Allergy Respir Dis. 2005. 15:408–414.9. Ciprandi G, Signori A, Tosca MA, Cirillo I. Bronchodilation test in patients with allergic rhinitis. Allergy. 2011. 66:694–698.10. Simon MR, Chinchilli VM, Phillips BR, Sorkness CA, Lemanske RF Jr, Szefler SJ, et al. Forced expiratory flow between 25% and 75% of vital capacity and FEV1/forced vital capacity ratio in relation to clinical and physiological parameters in asthmatic children with normal FEV1 values. J Allergy Clin Immunol. 2010. 126:527–534.e1-8.11. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005. 26:319–338.12. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005. 26:948–968.13. Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA) 2010. c2010. cited 2011 Sep 14. GINA;Available from: http://www.ginasthma.org/pdf/GINA_Report_2010.pdf.14. Sposato B, Mariotta S, Ricci A. When should a reversibility test be performed on patients with early stages of asthma and normal spirometry? J Asthma. 2008. 45:479–483.15. Scichilone N, Battaglia S, Olivieri D, Bellia V. The role of small airways in monitoring the response to asthma treatment: what is beyond FEV1? Allergy. 2009. 64:1563–1569.16. Mariotta S, Sposato B, Ricci A, Bruno P, Aquilini M, Mannino F. Reversibility test in the early stages of bronchial asthma. J Asthma. 2005. 42:487–491.17. Gelb AF, Williams AJ, Zamel N. Spirometry. FEV1 vs FEF25-75 percent. Chest. 1983. 84:473–474.18. Hansen JE, Sun XG, Wasserman K. Discriminating measures and normal values for expiratory obstruction. Chest. 2006. 129:369–377.19. Bellia V, Cibella F, Cuttitta G, Scichilone N, Mancuso G, Vignola AM, et al. Effect of age upon airway obstruction and reversibility in adult patients with asthma. Chest. 1998. 114:1336–1342.20. Chotirmall SH, Watts M, Branagan P, Donegan CF, Moore A, McElvaney NG. Diagnosis and management of asthma in older adults. J Am Geriatr Soc. 2009. 57:901–909.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of the Severity in Patients with Bronchial Asthma Using FEF25-75%
- Relationships between fractional exhaled nitric oxide levels and FEF25%-75% in children with asthma
- Small Airway Impairment and Bronchial Hyperresponsiveness in Asthma Onset
- Interpretation of Bronchodilator Response inPatients with Obstructive Airway Disease
- Fractional exhaled nitric oxide and forced expiratory flow between 25% and 75% of vital capacity in children with controlled asthma
