Invasive Pulmonary Aspergillosis Histologically Mimicking Mucormycosis
- Affiliations
-
- 1Department of Internal Medicine, KEPCO Medical Center, Seoul, Korea.
- 2Department of Pathology, KEPCO Medical Center, Seoul, Korea.
- 3Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, Kyung Hee University School of Medicine, Seoul, Korea. humanmd04@hanmail.net
- KMID: 2171368
- DOI: http://doi.org/10.12771/emj.2016.39.2.65
Abstract
- Differential diagnosis of invasive aspergillosis from other pulmonary fungal infections including mucormycosis is important because the treatment is pathogen-dependent. Clinically, invasive aspergillosis is often discriminated from other mold infections on the basis of typical histopathologic features in the biopsy specimen. However, biopsy alone is not always complete because different fungal species can display similar histopathologic features. Surrogate markers or molecular-based assays can be useful when the results of conventional diagnostic modalities are conflicting. Here, we present a case of invasive pulmonary aspergillosis histologically mimicking mucormycosis, which was confirmed by fungal polymerase chain reaction.
MeSH Terms
Figure
-
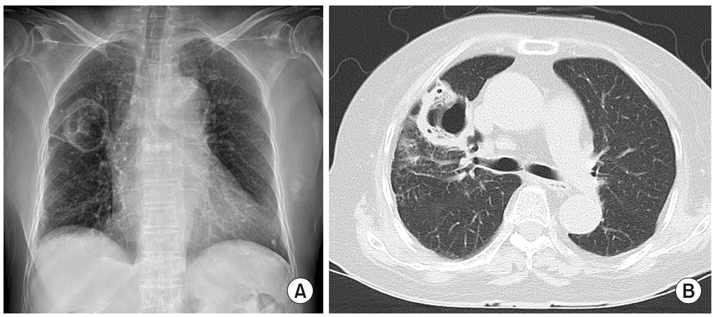
Fig. 1 Chest imaging at presentation. (A) Chest X-ray shows a 4 cm-sized cavitary lesion at right upper lobe. (B) Chest computed tomography scan reveals a thick, irregular-walled cavity at right upper lobe.
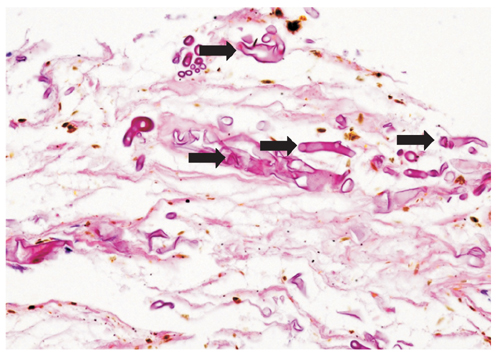
Fig. 2 Histopathologic image. In the biopsy specimen, non-septated and broad hyphae (arrows) with infiltration of inflammatory cells are detected. The finding is suspicious of mucormycosis (H&E, ×200).

Fig. 3 Polymerase chain reaction results using β-tubulin gene. Internal transcribed space and β-tubulin genes were used to identify isolate to the species complex level and to the species level within the complex, respectively. The sequences derived from those two genes were compared with sequences available in GenBank. The results confirmed that the isolate is 100% identical to Aspergillus fulmigatus.
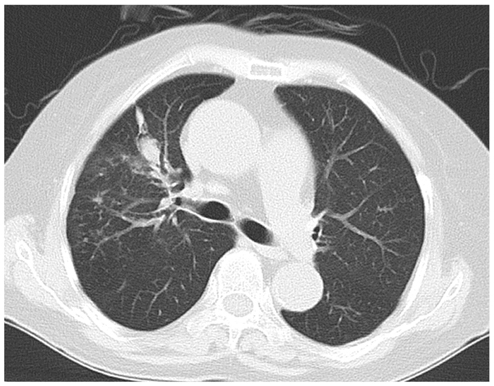
Fig. 4 Chest computed tomography scan after treatment with voriconazole. After 2 months of treatment, the lesion is markedly shrunken with remnant small consolidation.
Reference
-
1. Pfaller MA, Diekema DJ. Epidemiology of invasive mycoses in North America. Crit Rev Microbiol. 2010; 36:1–53.2. Ostrosky-Zeichner L. Invasive mycoses: diagnostic challenges. Am J Med. 2012; 125:1 Suppl. S14–S24.3. Marr KA, Carter RA, Crippa F, Wald A, Corey L. Epidemiology and outcome of mould infections in hematopoietic stem cell transplant recipients. Clin Infect Dis. 2002; 34:909–917.4. Legouge C, Caillot D, Chretien ML, Lafon I, Ferrant E, Audia S, et al. The reversed halo sign: pathognomonic pattern of pulmonary mucormycosis in leukemic patients with neutropenia? Clin Infect Dis. 2014; 58:672–678.5. Wahba H, Truong MT, Lei X, Kontoyiannis DP, Marom EM. Reversed halo sign in invasive pulmonary fungal infections. Clin Infect Dis. 2008; 46:1733–1737.6. Caillot D, Couaillier JF, Bernard A, Casasnovas O, Denning DW, Mannone L, et al. Increasing volume and changing characteristics of invasive pulmonary aspergillosis on sequential thoracic computed tomography scans in patients with neutropenia. J Clin Oncol. 2001; 19:253–259.7. Chandrasekar P. Diagnostic challenges and recent advances in the early management of invasive fungal infections. Eur J Haematol. 2010; 84:281–290.8. Hsu JL, Ruoss SJ, Bower ND, Lin M, Holodniy M, Stevens DA. Diagnosing invasive fungal disease in critically ill patients. Crit Rev Microbiol. 2011; 37:277–312.9. Cuenca-Estrella M, Meije Y, Diaz-Pedroche C, Gomez-Lopez A, Buitrago MJ, Bernal-Martinez L, et al. Value of serial quantification of fungal DNA by a real-time PCR-based technique for early diagnosis of invasive Aspergillosis in patients with febrile neutropenia. J Clin Microbiol. 2009; 47:379–384.10. Balajee SA, Houbraken J, Verweij PE, Hong SB, Yaghuchi T, Varga J, et al. Aspergillus species identification in the clinical setting. Stud Mycol. 2007; 59:39–46.11. Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. 2002; 347:408–415.12. Spellberg B, Edwards J Jr, Ibrahim A. Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin Microbiol Rev. 2005; 18:556–569.13. Lee S, Yun NR, Kim KH, Jeon JH, Kim EC, Chung DH, et al. Discrepancy between histology and culture in filamentous fungal infections. Med Mycol. 2010; 48:886–888.14. Pfeiffer CD, Fine JP, Safdar N. Diagnosis of invasive aspergillosis using a galactomannan assay: a meta-analysis. Clin Infect Dis. 2006; 42:1417–1427.15. Rickerts V, Mousset S, Lambrecht E, Tintelnot K, Schwerdtfeger R, Presterl E, et al. Comparison of histopathological analysis, culture, and polymerase chain reaction assays to detect invasive mold infections from biopsy specimens. Clin Infect Dis. 2007; 44:1078–1083.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Pulmonary Aspergillosis Invaded to Thoracic Vertebra in a Immunocompetent Host: A case report
- Diagnosis and Treatment of Invasive Mold Diseases
- A Case of chronic necrotizing pulmonary aspergillosis with pulmonary artery aneurysm
- Angioinvasive Mucormycosis Mimicking Mass and Pulmonary Thromboembolism in a Patient with Myelodysplastic Syndrome: A Case Report
- A Case of Endobronchial Aspergillosis Completely Obstructing Lobar Bronchus
