Bilateral Adrenocortical Masses Producing Aldosterone and Cortisol Independently
- Affiliations
-
- 1Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 2Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jaehyeon@skku.edu
- 3Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2169672
- DOI: http://doi.org/10.3803/EnM.2015.30.4.607
Abstract
- A 31-year-old woman was referred to our hospital with symptoms of hypertension and bilateral adrenocortical masses with no feature of Cushing syndrome. The serum aldosterone/renin ratio was elevated and the saline loading test showed no suppression of the plasma aldosterone level, consistent with a diagnosis of primary hyperaldosteronism. Overnight and low-dose dexamethasone suppression tests showed no suppression of serum cortisol, indicating a secondary diagnosis of subclinical Cushing syndrome. Adrenal vein sampling during the low-dose dexamethasone suppression test demonstrated excess secretion of cortisol from the left adrenal mass. A partial right adrenalectomy was performed, resulting in normalization of blood pressure, hypokalemia, and high aldosterone level, implying that the right adrenal mass was the main cause of the hyperaldosteronism. A total adrenalectomy for the left adrenal mass was later performed, resulting in a normalization of cortisol level. The final diagnosis was bilateral adrenocortical adenomas, which were secreting aldosterone and cortisol independently. This case is the first report of a concurrent cortisol-producing left adrenal adenoma and an aldosterone-producing right adrenal adenoma in Korea, as demonstrated by adrenal vein sampling and sequential removal of adrenal masses.
MeSH Terms
Figure
-
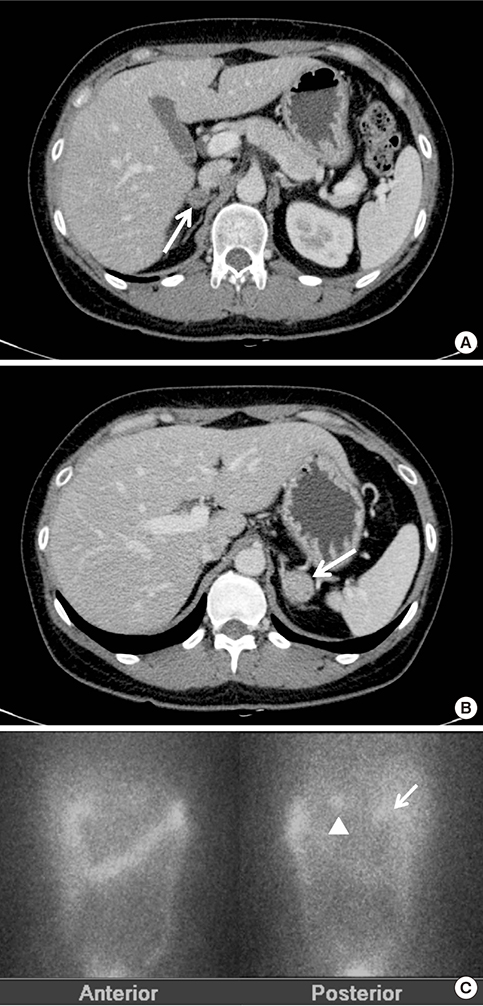
Fig. 1 Adrenal Images. (A, B) Adrenal computed tomography. Axial images showed bilateral adrenal masses (arrows), including a 1.6-cm mass on the right adrenal gland (A) and a 2-cm mass on the left (B). (C) Adrenal NP-59 scan demonstrated focally increased radioactive uptakes in the bilateral adrenal gland areas (arrow, arrowhead), especially on the left side (arrowhead).

Fig. 2 Adrenalectomy specimens (gross and microscopic findings). (A) The right adrenal mass was a 1.4×1.4×1.2-cm ovoid, bright yellow, and well-circumscribed mass arising from the cortex. (B) Microscopically, the right adrenal mass consisted primarily of clear cells (H&E stain, ×200). (C) The left adrenal mass was brown, solid in appearance, and encapsulated. (D) The left adrenal mass was composed of both clear cells and eosinophilic compact cells (H&E stain, ×200).
Cited by 1 articles
-
Adrenal Venous Sampling for Subtype Diagnosis of Primary Hyperaldosteronism
Mitsuhide Naruse, Akiyo Tanabe, Koichi Yamamoto, Hiromi Rakugi, Mitsuhiro Kometani, Takashi Yoneda, Hiroki Kobayashi, Masanori Abe, Youichi Ohno, Nobuya Inagaki, Shoichiro Izawa, Masakatsu Sone
Endocrinol Metab. 2021;36(5):965-973. doi: 10.3803/EnM.2021.1192.
Reference
-
1. Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf). 2007; 66:607–618.2. Kim SW. Primary aldosteronism. Korean J Med. 2012; 82:396–402.3. De Leo M, Cozzolino A, Colao A, Pivonello R. Subclinical Cushing's syndrome. Best Pract Res Clin Endocrinol Metab. 2012; 26:497–505.4. Terzolo M, Pia A, Reimondo G. Subclinical Cushing's syndrome: definition and management. Clin Endocrinol (Oxf). 2012; 76:12–18.5. Morelli V, Reimondo G, Giordano R, Della Casa S, Policola C, Palmieri S, et al. Long-term follow-up in adrenal incidentalomas: an Italian multicenter study. J Clin Endocrinol Metab. 2014; 99:827–834.6. Kempers MJ, Lenders JW, van Outheusden L, van der Wilt GJ, Schultze Kool LJ, Hermus AR, et al. Systematic review: diagnostic procedures to differentiate unilateral from bilateral adrenal abnormality in primary aldosteronism. Ann Intern Med. 2009; 151:329–337.7. Levinson PD, Zadik Z, Hamilton BP, Mersey JH, White RI, Kowarski AA. Adrenal vein epinephrine levels: a useful aid in venous sampling for primary aldosteronism. Ann Intern Med. 1982; 97:690–693.8. Lee JS, Kang MY, Kim SW, Shin CS, Kim SY, Chung JW. The clinical implication and problems of adrenal vein sampling in patients with primary aldosteronism. J Korean Endocr Soc. 2007; 22:428–435.9. Young WF Jr, du Plessis H, Thompson GB, Grant CS, Farley DR, Richards ML, et al. The clinical conundrum of corticotropin-independent autonomous cortisol secretion in patients with bilateral adrenal masses. World J Surg. 2008; 32:856–862.10. Ku EJ, Hong AR, Kim YA, Bae JH, Chang MS, Kim SW. Adrenocorticotropic hormone-independent cushing syndrome with bilateral cortisol-secreting adenomas. Endocrinol Metab (Seoul). 2013; 28:133–137.11. Cho YY, Suh S, Joung JY, Jeong H, Je D, Yoo H, et al. Clinical characteristics and follow-up of Korean patients with adrenal incidentalomas. Korean J Intern Med. 2013; 28:557–564.12. Wu VC, Chueh SC, Chang HW, Lin WC, Liu KL, Li HY, et al. Bilateral aldosterone-producing adenomas: differentiation from bilateral adrenal hyperplasia. QJM. 2008; 101:13–22.13. Fujimoto K, Honjo S, Tatsuoka H, Hamamoto Y, Kawasaki Y, Matsuoka A, et al. Primary aldosteronism associated with subclinical Cushing syndrome. J Endocrinol Invest. 2013; 36:564–567.14. Hiraishi K, Yoshimoto T, Tsuchiya K, Minami I, Doi M, Izumiyama H, et al. Clinicopathological features of primary aldosteronism associated with subclinical Cushing's syndrome. Endocr J. 2011; 58:543–551.15. Oki K, Yamane K, Sakashita Y, Kamei N, Watanabe H, Toyota N, et al. Primary aldosteronism and hypercortisolism due to bilateral functioning adrenocortical adenomas. Clin Exp Nephrol. 2008; 12:382–387.16. Choi SE, Kim YC, Noh DY, Youn YK, Oh SK. A case of bilateral adrenal cortical adenomas causing Cushing's syndrome and primary aldosteronism. J Korean Surg Soc. 1998; 55:769–774.17. Nagae A, Murakami E, Hiwada K, Kubota O, Takada Y, Ohmori T. Primary aldosteronism with cortisol overproduction from bilateral multiple adrenal adenomas. Jpn J Med. 1991; 30:26–31.18. Okura T, Miyoshi K, Watanabe S, Kurata M, Irita J, Manabe S, et al. Coexistence of three distinct adrenal tumors in the same adrenal gland in a patient with primary aldosteronism and preclinical Cushing's syndrome. Clin Exp Nephrol. 2006; 10:127–130.19. Onoda N, Ishikawa T, Nishio K, Tahara H, Inaba M, Wakasa K, et al. Cushing's syndrome by left adrenocortical adenoma synchronously associated with primary aldosteronism by right adrenocortical adenoma: report of a case. Endocr J. 2009; 56:495–502.20. Lack EE, Wieneke J. Chapter 19, Tumors of the adrenal gland. Diagnostic histopathology of tumors. 4th ed. Philadelphia: Elsevier Health Sciences;2013. p. 1294–1325.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Aldosterone-Producing Adrenocortical Carcinoma without Hypertension
- A Case of Adrenocortical Carcinoma Secreting Cortisol, Androgen and Aldosterone
- A Case Report of an Aldosterone-producing Adrenocortical Carcinoma
- A case of adrenocortical adenoma with primary hyperaldosteronism and subclinical Cushing's syndrome
- A case of idiopathic hyperaldosteronism vs. bilateral aldosterone producing adenoma
