Endocrinol Metab.
2011 Sep;26(3):239-242. 10.3803/EnM.2011.26.3.239.
A Case of Adrenocortical Carcinoma Secreting Cortisol, Androgen and Aldosterone
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Kyung Hee University, Seoul, Korea. chy1009@hotmail.com
- 2College of Nursing, Sungshin Women's University, Seoul, Korea.
- KMID: 2169175
- DOI: http://doi.org/10.3803/EnM.2011.26.3.239
Abstract
- Primary adrenocortical carcinoma is a rare tumor, and is characterized by a peri-tumor mass effect and hormone excess signs. Adrenocortical carcinoma most commonly secretes cortisol, but tumors that secrete other adrenal hormones (aldosterone, androgen) are rare. Herein, we report the case of a 70-year-old woman with cortisol, androgen, and aldosterone-secreting adrenal carcinoma. The patient complained of generalized weakness, moon face, and central obesity. On laboratory examination, hypokalemia and metabolic alkalosis was detected. On the hormone test, cortisol, DHEA-S, and aldosterone were all increased. Abdominal CT showed a large right adrenal mass. She underwent right adrenalectomy and the histology revealed the presence of an adrenocortical carcinoma. After adrenalectomy, the patient was treated with hydrocortisone and mitotane.
MeSH Terms
Figure
-

Fig. 1 Abdominal CT scan showing a large right adrenal mass (maxinum diameter, 10 cm).
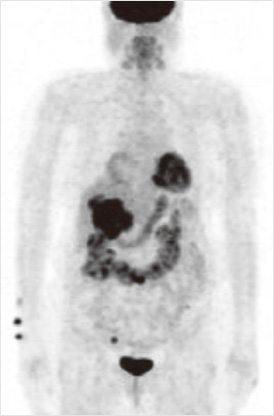
Fig. 2 PET-CT shows highly active lesion in right adrenal area.
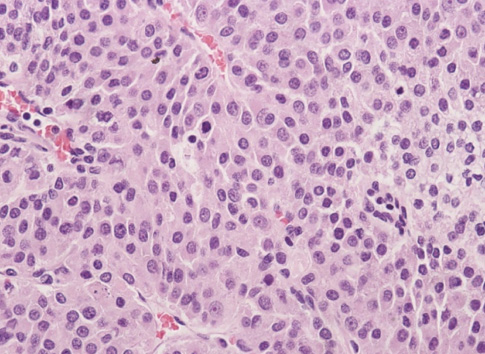
Fig. 3 Microscopic findings of the surgically removed tumor (H&E stain, × 400).
Reference
-
1. Allolio B, Fassnacht M. Clinical review: Adrenocortical carcinoma: clinical update. J Clin Endocrinol Metab. 2006. 91:2027–2037.2. Wajchenberg BL, Albergaria Pereira MA, Medonca BB, Latronico AC, Campos Carneiro P, Alves VA, Zerbini MC, Liberman B, Carlos Gomes G, Kirschner MA. Adrenocortical carcinoma: clinical and laboratory observations. Cancer. 2000. 88:711–736.3. Dackiw AP, Lee JE, Gagel RF, Evans DB. Adrenal cortical carcinoma. World J Surg. 2001. 25:914–926.4. Bilimoria KY, Shen WT, Elaraj D, Bentrem DJ, Winchester DJ, Kebebew E, Sturgeon C. Adrenocortical carcinoma in the United States: treatment utilization and prognostic factors. Cancer. 2008. 113:3130–3136.5. Libe R, Fratticci A, Bertherat J. Adrenocortical cancer: pathophysiology and clinical management. Endocr Relat Cancer. 2007. 14:13–28.6. Allolio B, Hahner S, Weismann D, Fassnacht M. Management of adrenocortical carcinoma. Clin Endocrinol (Oxf). 2004. 60:273–287.7. Peppa M, Pikounis V, Papaxoinis G, Macheras A, Economopoulos T, Raptis SA, Hadjidakis D. Adrenocortical carcinoma secreting cortisol, androgens and aldosterone: a case report. Cases J. 2009. 2:8951.8. Lee CW, Yoon HJ, Hwang WM, Kim JK, Koo HS, Lim DM, Choi EG, Na MJ, Cho DY, Kim BK, Choi IS, Park KY. A case of adrenocortical carcinoma with concurrent Cushing's syndrome and primary aldosteronism. J Korean Soc Endocrinol. 2004. 19:446–451.9. Stojadinovic A, Ghossein RA, Hoos A, Nissan A, Marshall D, Dudas M, Cordon-Cardo C, Jaques DP, Brennan MF. Adrenocortical carcinoma: clinical, morphologic, and molecular characterization. J Clin Oncol. 2002. 20:941–950.10. Seccia TM, Fassina A, Nussdorfer GG, Pessina AC, Rossi GP. Aldosterone-producing adrenocortical carcinoma: an unusual cause of Conn's syndrome with an ominous clinical course. Endocr Relat Cancer. 2005. 12:149–159.11. Kendrick ML, Curlee K, Lloyd R, Farley DR, Grant CS, Thompson GB, Rowland C, Young WF Jr, van Heerden JA. Aldosterone-secreting adrenocortical carcinomas are associated with unique operative risks and outcomes. Surgery. 2002. 132:1008–1011. discussion 1012.12. Derksen J, Nagesser SK, Meinders AE, Haak HR, van de Velde CJ. Identification of virilizing adrenal tumors in hirsute women. N Engl J Med. 1994. 331:968–973.13. Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004. 25:309–340.14. Szolar DH, Korobkin M, Reittner P, Berghold A, Bauernhofer T, Trummer H, Schoellnast H, Preidler KW, Samonigg H. Adrenocortical carcinomas and adrenal pheochromocytomas: mass and enhancement loss evaluation at delayed contrast-enhanced CT. Radiology. 2005. 234:479–485.15. Outwater EK, Siegelman ES, Huang AB, Birnbaum BA. Adrenal masses: correlation between CT attenuation value and chemical shift ratio at MR imaging with in-phase and opposed-phase sequences. Radiology. 1996. 200:749–752.16. Macfarlane DA. Cancer of the adrenal cortex; the natural history, prognosis and treatment in a study of fifty-five cases. Ann R Coll Surg Engl. 1958. 23:155–186.17. Vassilopoulou-Sellin R, Schultz PN. Adrenocortical carcinoma. Clinical outcome at the end of the 20th century. Cancer. 2001. 92:1113–1121.18. Didolkar MS, Bescher RA, Elias EG, Moore RH. Natural history of adrenal cortical carcinoma: a clinicopathologic study of 42 patients. Cancer. 1981. 47:2153–2161.19. Fassnacht M, Hahner S, Polat B, Koschker AC, Kenn W, Flentje M, Allolio B. Efficacy of adjuvant radiotherapy of the tumor bed on local recurrence of adrenocortical carcinoma. J Clin Endocrinol Metab. 2006. 91:4501–4504.
