Korean J Hematol.
2005 Dec;40(4):261-265. 10.5045/kjh.2005.40.4.261.
A Case of Multiple Myeloma Presenting as Non-obstructive Jaundice Due to Plasma Cell Infiltration of the Liver
- Affiliations
-
- 1Department of Internal Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. sklee2@amc.seoul.kr
- 2Department of Pathology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 2083464
- DOI: http://doi.org/10.5045/kjh.2005.40.4.261
Abstract
- Extraosseous manifestations are found in less than 5% of the patients with multiple myeloma. We reported here on a rare case of multiple myeloma presenting as non-obstructive jaundice due to diffuse plasma cell infiltration of the liver. A 70-year-old man was referred to our hospital because of general weakness, weight loss, jaundice, anemia and proteinuria. The laboratory studies showed: hemoglobin 8.5g/dL, calcium 10.3mg/dL, creatinine 1.3mg/dL, AST 41IU/L, ALT 26IU/L, alkaline phosphatase 304IU/L, total bilirubin 4.0mg/dL, direct bilirubin 2.3mg/dL and 24 hour urinary protein 1,120mg. The serologic tests for hepatitis B and C virus were negative. The abdominal CT scans were normal. The urinary protein studies revealed a M component of the lamda type light chain. The bone marrow biopsy showed atypical plasma cells, and the liver biopsy showed a diffuse sinusoidal infiltration of plasma cells.
Keyword
MeSH Terms
Figure
-
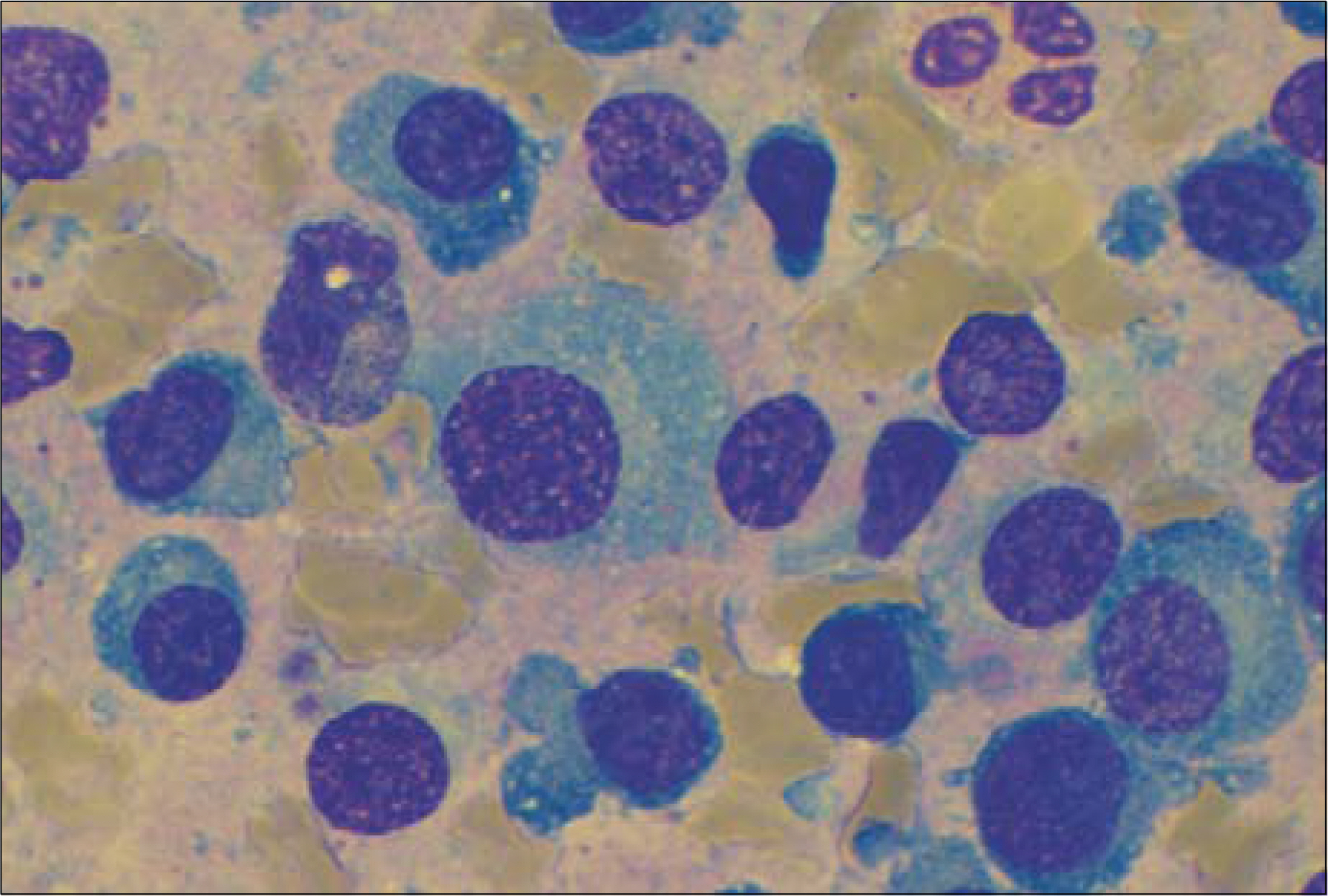
Fig. 1. Neoplastic plasma cells (in bone marrow) show abundant deep-blue cytoplasm with perinuclear halo (Wright-Giemsa stain, ×1,000).
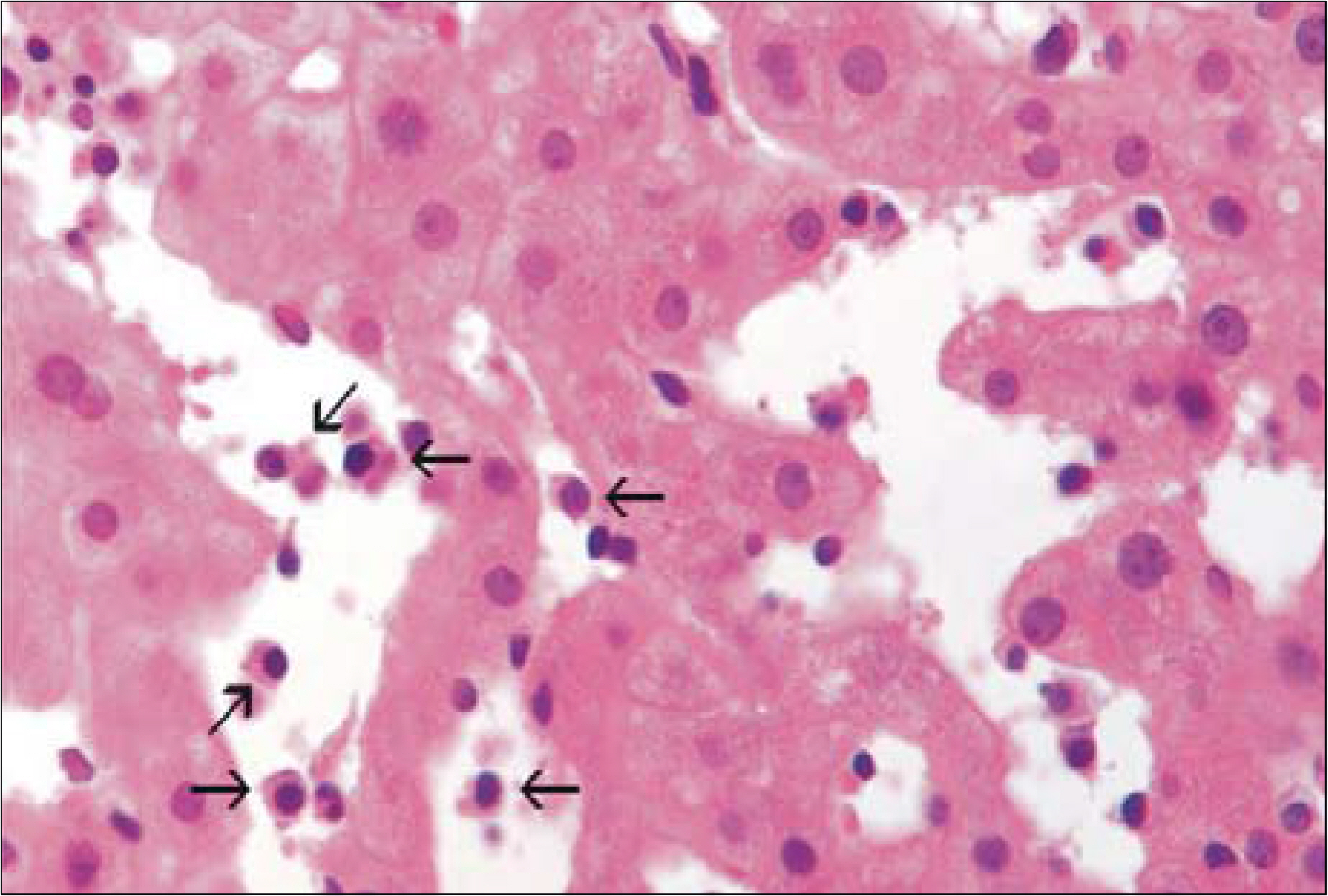
Fig. 2. The infiltrated myeloma cells are seen in dilated sinusoids (H & E stain, ×400).
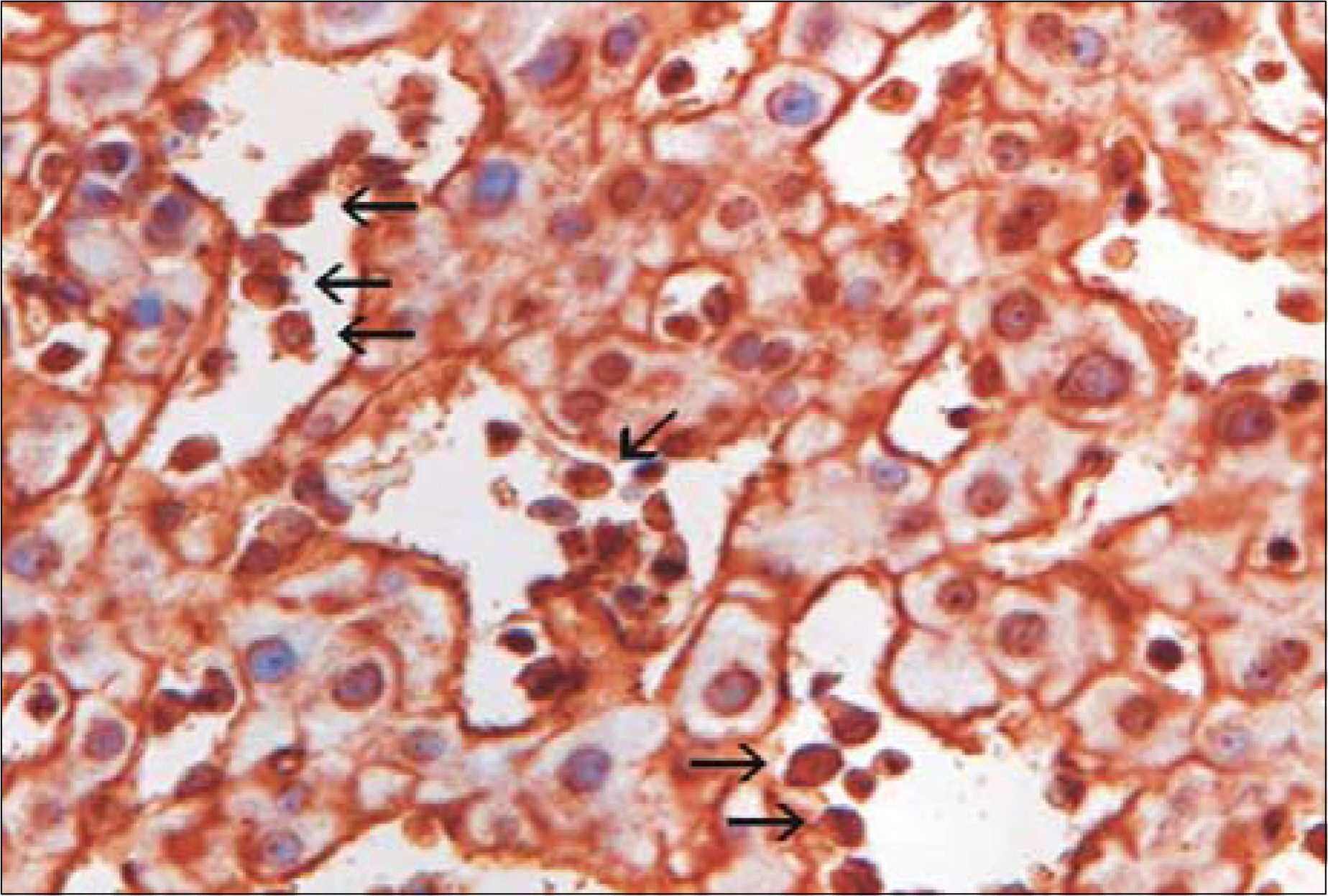
Fig. 3. The immunostains for CD 138, myeloma cells show intense cytoplasmic reactivity, but surrounding hepatocytes does not (×400).
Reference
-
1). Kapadia SB. Multiple myeloma: a clinicopathologic study of 62 consecutively autopsied cases. Medicine (Baltimore). 1980; 59:380–92.2). Moulopoulos LA, Granfield CA, Dimopoulos MA, Kim EE, Alexanian R, Libshitz HI. Extraosseous multiple myeloma: imaging features. ARJ. 1993; 161:1083–7.
Article3). Thomas FB, Clausen KP, Greenberger NJ. Liver disease in multiple myeloma. Arch Intern Med. 1973; 132:195–202.
Article4). Fischer A, Suhrland M, Vogl SE. Myeloma of the head of the pancreas: a case report. Cancer. 1991; 67:681–3.
Article5). Michopoulos S, Petraki K, Petraki C, Dimopoulos MA. Light chain deposition disease of the liver without renal involvement in a patient with multiple myeloma related to liver failure and rapid fatal outcome. Digestive Disease and Sciences. 2002; 47:730–4.6). Yoon YS, Yoo HM, Chon CY, et al. Liver involvement in multiple myelola proven by peritoneoscopy: a case report. Yonsei Med J. 1993; 34:90–7.7). Pastor E, Perella M, Gomez A, Grau E, Perez A, Escandon J. Multiple myeloma of the liver pre-senting as nonobstructive jaundice. Am J Hematol. 1996; 53:205–6.
Article8). Arebi N, Patel B, Aqel NM, Pitcher MCL. IgA multiple myeloma presenting as non-obstructive jaundice. Postgrad Med J. 2004; 80:489–90.
Article9). Stegman R, Alexanian R. Solid tumors in multiple myeloma. Ann Intern Med. 1979; 90:780–2.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Liver Involvement in Multiple Myeloma Proven by Peritoneoscopy
- A Case of Multiple Myeloma with Multiple Intrahepatic Extramedullary Plasmacytomas
- A Case of Multiple Myeloma in Bilateral Paranasal Sinuses with Loss of Vision
- SOLITARY PLASMA CELL MYELOMA ON ANTERIOR MAXILLA: A CASE REPORT
- A Case of Multiple Myeloma First Presenting as Cutaneous Plasmacytoma
