An Adenocarcinoma of Lung with Unusual Very Slow Growth : A case report
- Affiliations
-
- 1Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, College of Medicine, Pochon CHA University, Seongnam, Korea.
- 2Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, College of Medicine, Korea University, Seoul, Korea. khin@korea.ac.kr
- 3Department of Radiology, College of Medicine, Korea University, Seoul, Korea.
- 4Department of Pathology, College of Medicine, Korea University, Seoul, Korea.
- KMID: 1881527
- DOI: http://doi.org/10.6058/jlc.2006.5.1.51
Abstract
- The prognosis of lung cancer is very poor. Patients with lung cancer have usually no symptom in early stage or some mild cough, sputum. When patient feel weight loss or dyspnea, majority of patients with lung cancer are advanced stage and inoperable. The growth rate of lung cancer is different according to cell type of tumor and related to prognosis. Generally, tumor. doubling time (TDT) of lung cancer has been known that small cell lung cancer is about 65 days, squamous cell carcinoma is about 90 days, and adenocarcinoma is about 185 days. There has been rarely reported of lung cancer with very fast or very slow growth. The prognosis of a slow growing lung cancer is relatively good but rapidly growing cancer is not. We report a very rare case that surgicallytreated early stage non-small cell lung cancer (adenocarcinoma) with 4-year- TDT without invasion or distant metastasis
Keyword
MeSH Terms
Figure
-

Fig. 1. Chest radiography (A) and HRCT scan (B) at initial presentation, demonstrating a well-defined mult卜septated cavitary lung lesion in the superior segment of the right lower lobe.
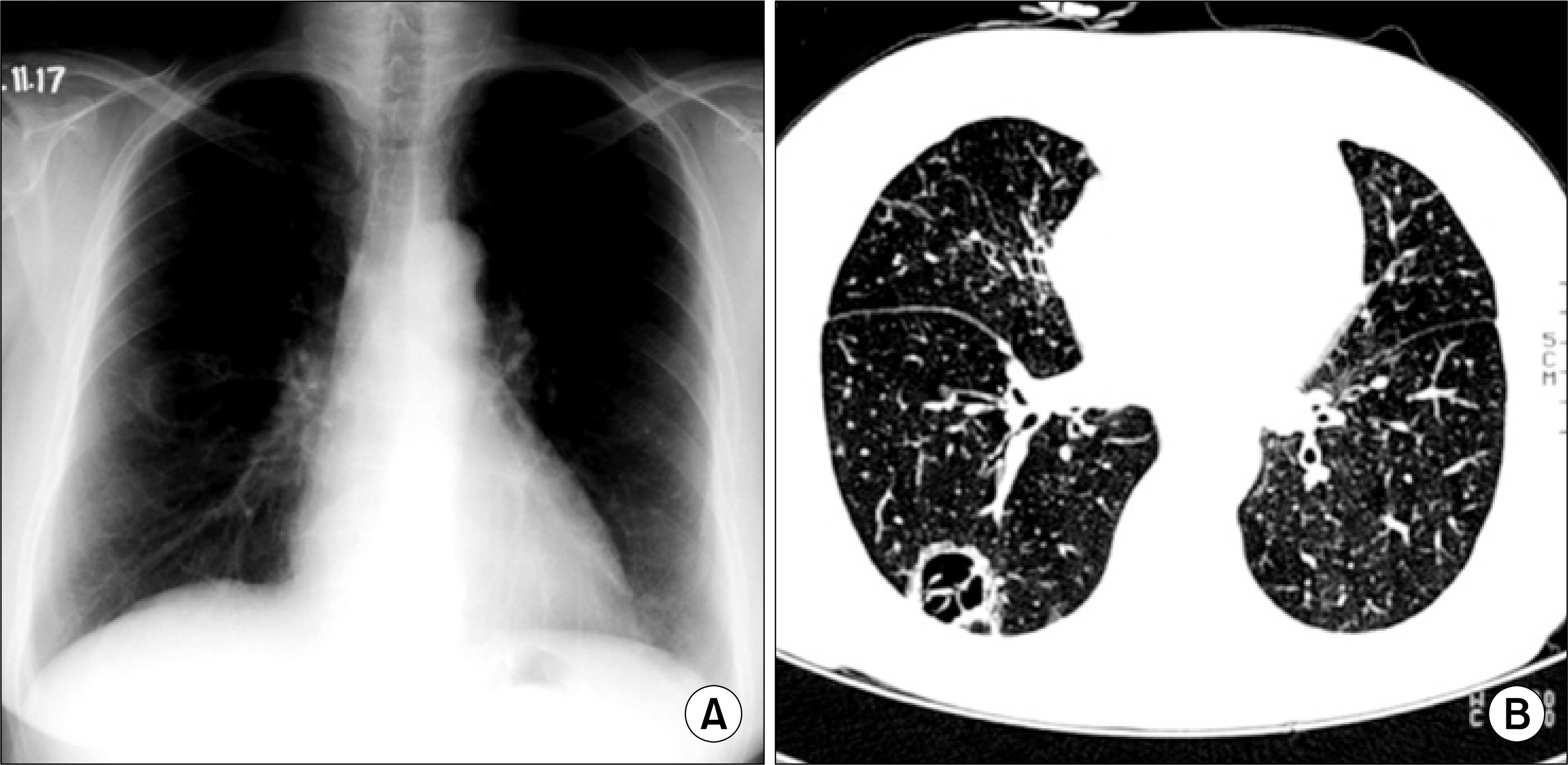
Fig. 2. Chest radiography (A) and HRCT scan (B) taken 2 years later, demonstrating that the size of lung mass had increased slightly.

Fig. 3. Chest radiography (A) and HRCT scan (B) taken 8 years after the initial presentation showing that the cavitary lung mass had increased in size and developed a solid portion.

Fig. 4. Percutaneous transthoracic needle aspiration of lung. Hematoxylin and Eosin (H&E) stain (x 400). The cell-block slide showed a few clusters of atypical cells with irregular nuclei and moderate amounts of cytoplasm, suggestive of adenocarcinoma.

Fig. 5. Gross finding of lung cancer in the right lower lobe, during lobectomy.

Fig. 6. Well differentiated adenocarcinoma of the lung, showing a bronchi㢌oalveᄋlar carcinoma-like growth pattern with atypical cells lining the alveolar wall (H&E stain, x400).
Reference
-
1.Freiberg S., Mattso S. On the growth rates of human malignant tumors: implications for medical decision making. J Surg Oncol. 1997. 65:784–797.2.Yamaguchi M: Sugio K: Ondo K, et al. Slowly progressive adenocarcinoma of the lung: report case. Ann Thorac Cardiovasc Surg. 2002. 8:160–162.3.Ching-Lih S., Yu-Chin L., Reury-Pcmg P. Fast-growing squamous cell lung cancer. Lung Cancer. 2002. 36:199–202.
Article4.Schwartz M. A biomathmatical approach to clinical tumor growth. Cancer. 1961. 14:1272–1294.5.Mattem J., Volm M. Clinical estimation of the growth rate of lung cancer. Anticancer Res. 2001. 21:4067–4070.6.Hasegawa M., Sone S: Takashima S, et al. Growth rate of small lung cancers detected on mass CT screening. Br J Radiol. 2000. 73:1252–1259.
Article7.Takatoshi A., Hajime N., Hideyuki W, et al. Evolution of peripheral lung adenocarcinomas: CT findings correlated with histology and tumor doubling time. AJR. 2000. 174:763–768.8.Morihito 0., Wataru N., Toshihiko S, et al. Correlation between computed tomographic findings, bronchioloalveolar carcinoma component, and biologic behavior of small sized lung adenocarcinomas. J Thorac Cardiovasc Surg. 2004. 127:857–861.9.Wang JC: Sone S., Feng L, et al. Rapidly growing small peripheral lung cancers detected by screening CT: correlation between radiological appearance and pathological features. Br J Radiol. 2000. 73:930–937.10.Noguchi M., Morikawa A., Kawasaki M, et al. Small adenocarcinoma of the lung. Cancer. 1995. 75:2844–2852.11.Aquino SL: Chiles C: Halford P. Distinction of consolidative bronchioloalveolar carcinoma from pneumonia: do CT criteria work? AJR. 1998. 171:359–363.12.Hill CA. Bronchiolo-alveolar carcinoma: a review. Radiology. 1984. 150:15–20.
Article13.Strollo DC., Rosado-de-Christenson ML., Franks TJ. Reclassification of cystic bronchioloalveolar carcinomas to adenocarcinomas to adenocarcinomas based on the revised world health organization classification of lung and pleural tumors. J Thorac Imaging. 2003. 18:59–66.14.Yoshida T: Harada T., Fuke S, et al. Lung adenocarcinoma presenting with enlarged and multiloculated cystic lesions over 2 years. Respir Care. 2004. 49:1522–1524.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ovarian and Pituitary Metastasis from Adenocarcinoma of the Lung: A Case Report
- A Case of Zosterifom Cutaneous Metastatic Carcinoma
- Successful Rechallenge with Gefitinib for an Initial Erlotinib-Responder with Advanced Lung Adenocarcinoma
- Morphological Features of the Most Advanced Intra-Tumor Component in Multistep Progression
- A Case of Hyperamylasemia Associated with Lung Adenocarcinoma
