Diabetes Metab J.
2015 Apr;39(2):126-131. 10.4093/dmj.2015.39.2.126.
Clinical Features and Causes of Endogenous Hyperinsulinemic Hypoglycemia in Korea
- Affiliations
-
- 1Department of Internal Medicine, University of Ulsan College of Medicine, Seoul, Korea. kulee@amc.seoul.kr
- 2Department of Statistics, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1805895
- DOI: http://doi.org/10.4093/dmj.2015.39.2.126
Abstract
- BACKGROUND
Endogenous hyperinsulinemic hypoglycemia (EHH) is characterized by an inappropriately high plasma insulin level, despite a low plasma glucose level. Most of the EHH cases are caused by insulinoma, whereas nesidioblastosis and insulin autoimmune syndrome (IAS) are relatively rare.
METHODS
To evaluate the relative frequencies of various causes of EHH in Korea, we retrospectively analyzed 84 patients who were diagnosed with EHH from 1998 to 2012 in a university hospital.
RESULTS
Among the 84 EHH patients, 74 patients (88%), five (6%), and five (6%) were diagnosed with insulinoma, nesidioblastosis or IAS, respectively. The most common clinical manifestation of EHH was neuroglycopenic symptoms. Symptom duration before diagnosis was 14.5 months (range, 1 to 120 months) for insulinoma, 1.0 months (range, 6 days to 7 months) for nesidioblastosis, and 2.0 months (range, 1 to 12 months) for IAS. One patient, who was diagnosed with nesidioblastosis in 2006, underwent distal pancreatectomy but was later determined to be positive for insulin autoantibodies. Except for one patient who was diagnosed in 2007, the remaining three patients with nesidioblastosis demonstrated severe hyperinsulinemia (157 to 2,719 microIU/mL), which suggests that these patients might have had IAS, rather than nesidioblastosis.
CONCLUSION
The results of this study suggest that the prevalence of IAS may be higher in Korea than previously thought. Therefore, measurement of insulin autoantibody levels is warranted for EHH patients, especially in patients with very high plasma insulin levels.
Keyword
MeSH Terms
Figure
-
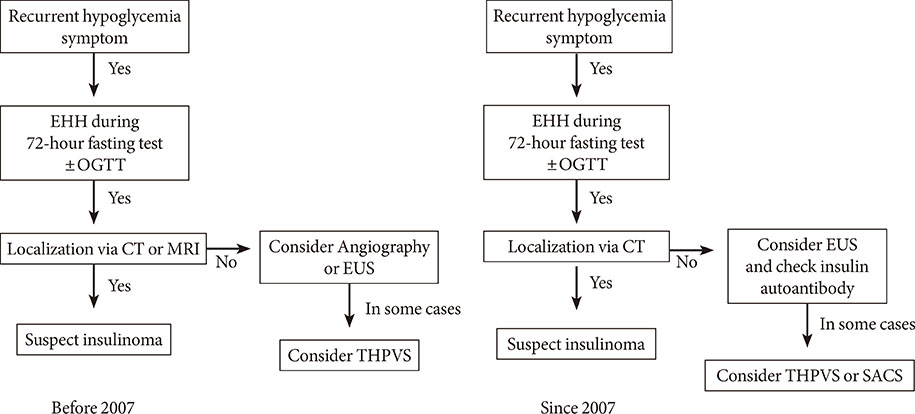
Fig. 1 Flow diagram of the localization strategies used to identify endogenous hyperinsulinemic hypoglycemia (EHH) patients. OGTT, oral glucose tolerance test; CT, computed tomography; MRI, magnetic resonance imaging; EUS, endoscopic ultrasound; THPVS, trans-hepatic portal vein sampling; SACS, selective arterial calcium stimulation.

Fig. 2 Plasma insulin levels in patients diagnosed with insulinoma, nesidioblastosis, and insulin autoimmune syndrome (IAS). The case indicted by the arrow demonstrated positive results on the insulin autoantibody test (3,000 µIU/mL, case no. 9 in Table 2). The other case indicated by the head of arrow demonstrated negative results on the insulin autoantibody test (5 µIU/mL, case no. 10 in Table 2).
Reference
-
1. Service FJ. Diagnostic approach to adults with hypoglycemic disorders. Endocrinol Metab Clin North Am. 1999; 28:519–532.2. Grant CS. Insulinoma. Best Pract Res Clin Gastroenterol. 2005; 19:783–798.3. Service FJ. Hypoglycemic disorders. N Engl J Med. 1995; 332:1144–1152.4. Service GJ, Thompson GB, Service FJ, Andrews JC, Collazo-Clavell ML, Lloyd RV. Hyperinsulinemic hypoglycemia with nesidioblastosis after gastric-bypass surgery. N Engl J Med. 2005; 353:249–254.5. Anlauf M, Wieben D, Perren A, Sipos B, Komminoth P, Raffel A, Kruse ML, Fottner C, Knoefel WT, Monig H, Heitz PU, Kloppel G. Persistent hyperinsulinemic hypoglycemia in 15 adults with diffuse nesidioblastosis: diagnostic criteria, incidence, and characterization of beta-cell changes. Am J Surg Pathol. 2005; 29:524–533.6. Lupsa BC, Chong AY, Cochran EK, Soos MA, Semple RK, Gorden P. Autoimmune forms of hypoglycemia. Medicine (Baltimore). 2009; 88:141–153.7. Uchigata Y, Hirata Y, Iwamoto Y. Insulin autoimmune syndrome (Hirata disease): epidemiology in Asia, including Japan. Diabetol Int. 2010; 1:21–25.8. Uchigata Y, Eguchi Y, Takayama-Hasumi S, Omori Y. Insulin autoimmune syndrome (Hirata disease): clinical features and epidemiology in Japan. Diabetes Res Clin Pract. 1994; 22:89–94.9. Park HJ, Park JY, Shong YK, Hong SK, Lee KU, Han DJ, Sung KB, Kim GS. Clinical manifestation of 16 cases with insulinoma or nesidioblastosis. Korean J Med. 1999; 56:189–195.10. Rindi G, Solcia E. Endocrine hyperplasia and dysplasia in the pathogenesis of gastrointestinal and pancreatic endocrine tumors. Gastroenterol Clin North Am. 2007; 36:851–865.11. Raffel A, Krausch MM, Anlauf M, Wieben D, Braunstein S, Kloppel G, Roher HD, Knoefel WT. Diffuse nesidioblastosis as a cause of hyperinsulinemic hypoglycemia in adults: a diagnostic and therapeutic challenge. Surgery. 2007; 141:179–184.12. Virally ML, Guillausseau PJ. Hypoglycemia in adults. Diabetes Metab. 1999; 25:477–490.13. Redmon JB, Nuttall FQ. Autoimmune hypoglycemia. Endocrinol Metab Clin North Am. 1999; 28:603–618.14. Ma WY, Won JG, Tang KT, Lin HD. Severe hypoglycemic coma due to insulin autoimmune syndrome. J Chin Med Assoc. 2005; 68:82–86.15. Kaczirek K, Niederle B. Nesidioblastosis: an old term and a new understanding. World J Surg. 2004; 28:1227–1230.16. McHenry C, Newell K, Chejfec G, Barbato A, Lawrence AM, Brooks M, Emanuele MA, Paloyan E. Adult nesidioblastosis. An unusual cause of fasting hypoglycemia. Am Surg. 1989; 55:366–369.17. Fong TL, Warner NE, Kumar D. Pancreatic nesidioblastosis in adults. Diabetes Care. 1989; 12:108–114.18. Jabri AL, Bayard C. Nesidioblastosis associated with hyperinsulinemic hypoglycemia in adults: review of the literature. Eur J Intern Med. 2004; 15:407–410.19. Patti ME, Goldfine AB. Hypoglycaemia following gastric bypass surgery: diabetes remission in the extreme? Diabetologia. 2010; 53:2276–2279.20. Goldfine AB, Mun EC, Devine E, Bernier R, Baz-Hecht M, Jones DB, Schneider BE, Holst JJ, Patti ME. Patients with neuroglycopenia after gastric bypass surgery have exaggerated incretin and insulin secretory responses to a mixed meal. J Clin Endocrinol Metab. 2007; 92:4678–4685.21. Uchigata Y, Hirata Y. Insulin autoimmune syndrome (IAS, Hirata disease). Ann Med Interne (Paris). 1999; 150:245–253.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Hyperinsulinemic Hypoglycemia
- A Case of Hyperinsulinemic Hypoglycemia in Premature Infant Treated with Oral Diazoxide
- Nesidioblastosis in Neonate with Persistent Hyperinsulinemic Hypoglycemia
- Nesidioblastosis in an Elderly Patient with Hyperinsulinemic Hypoglycemia
- Nesidioblastosis with Hyperinsulinemic Hypoglycemia in Adult
