Successful Treatment of Pneumonia caused by Aspergillus terrerus and Cytomegalovirus after Chemotherapy for Acute Myelogenous Leukemia
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. symonlee@catholic.ac.kr
- KMID: 1782395
- DOI: http://doi.org/10.3947/ic.2012.44.1.26
Abstract
- We report a case of pneumonia caused by Aspergillus terreus and cytomegalovirus (CMV) in a patient with acute myleogenous leukemia (AML) after remission induction chemotherapy. A 19-year-old woman underwent chemotherapy for AML. Twenty-three days after completing chemotherapy, she experienced a neutropenic fever with a rapidly-progressive pulmonary infiltration. In those days, her serum galactomannan immunoassay was 4.7 and she was treated with intravenous voriconazole (6 mg/kg q12h for 2 doses, followed by 4 mg/kg q12h) because of persistent fever and radiological worsening, despite the administration of amphotericin B deoxycholate (1 mg/kg q24h) for 7 days. A chest CT showed wedge-shaped consolidation with a central hypodense lesion and an air-crescent sign in the right middle lobe. With maintenance therapy of oral voriconazole for 10 weeks, a partial response was shown and neutrophil count was still less than 100/mm3. A lobectomy of the right middle lobe was performed. A. terreus was discovered from the lung tissue. At the same time, giant cells with intranuclear inclusions were found and immunohistochemical staining for CMV was positive. Ganciclovir (5 mg/kg q12h) was added to voriconazole therapy for 3 weeks after surgery, and then cord blood hematopoietic stem cell transplantation (HSCT) was performed. During HSCT, foscarnet (60 mg/kg q12h) was substituted for ganciclovir, and both antiviral agents were used alternatively due to CMV DNAemia. After 83 days from HSCT, the patient achieved successful engraftment and discharged without worsening the pneumonia.
Keyword
MeSH Terms
-
Amphotericin B
Antiviral Agents
Aspergillus
Cytomegalovirus
Deoxycholic Acid
Drug Combinations
Female
Fetal Blood
Fever
Foscarnet
Ganciclovir
Giant Cells
Hematopoietic Stem Cell Transplantation
Humans
Immunoassay
Intranuclear Inclusion Bodies
Leukemia
Leukemia, Myeloid, Acute
Lung
Mannans
Neutrophils
Pneumonia
Pyrimidines
Remission Induction
Thorax
Triazoles
Young Adult
Amphotericin B
Antiviral Agents
Deoxycholic Acid
Drug Combinations
Foscarnet
Ganciclovir
Mannans
Pyrimidines
Triazoles
Figure
-
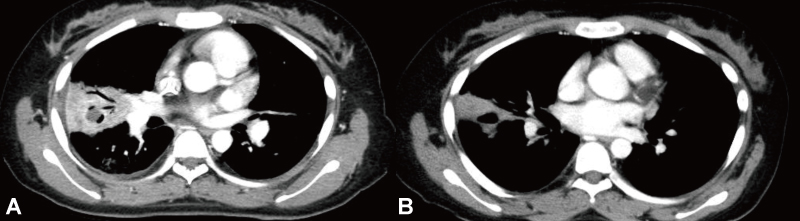
Figure 1 (A) Chest CT shows a wedge-shaped consolidation with focal necrosis and a central cavitary lesion on the right middle lobe. (B) On a follow-up chest CT after 10 weeks of voriconazole therapy, consolidation still remains with a focal necrosis and central cavitary lesion in the right middle lobe.

Figure 2 On hematoxylin-eosin staining, lung tissue from the cavitary lesion shows central hemorrhagic necrosis with infiltration of acute inflammatory cells (insertion: filamentous, branching septated hyphae within the necrotic tissue, Periodic Acid Schiff stain, ×400).
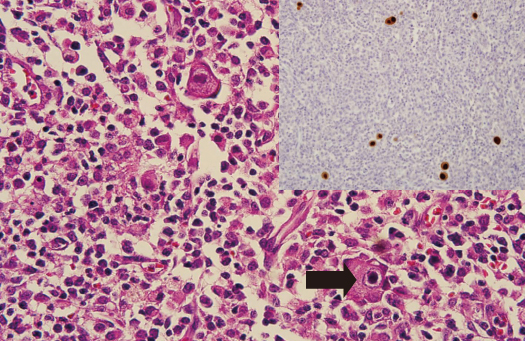
Figure 3 Lung specimen from the area of the cavitary lesion shows giant cells with intranuclear inclusions and a perinuclear halo (arrow, hematoxylin-eosin stain, ×400) (insertion: on immunohistochemistry lung biopsy specimen from the cavitary lesion shows CMV-virus-positive cells stained brown).
Reference
-
1. Donowitz GR, Maki DG, Crnich CJ, Pappas PG, Rolston KV. Infections in the neutropenic patient--new views of an old problem. Hematology Am Soc Hematol Educ Program. 2001:113–139.2. Vigil KJ, Adachi JA, Chemaly RF. Viral penumonias in immunocompromised adult hosts. J Intensive Care Med. 2010. 25:307–326.3. Razonable RR. Strategies for managing cytomegalovirus in transplant recipients. Expert Opin Pharmacother. 2010. 11:1983–1997.
Article4. Snydman DR, Limaye AP, Potena L, Zamora MR. Update and review: state-of-the-art management of cytomegalovirus infection and disease following thoracic organ transplantation. Transplant Proc. 2011. 43:3 Suppl. S1–S17.
Article5. Varani S, Landini MP. Cytomegalovirus-induced immunopathology and its clinical consequences. Herpesviridae. 2011. 2:6.
Article6. Kim GB, Choi SM, Lee DG, Kim HR, Lee KW, Nam KW, Kwok SK, Son DK, Chang JH, Choi JH, Shin WS, Kim CC. Human cytomegalovirus pneumonia and pulmonary aspergillosis in a patient with acute myelogenous leukemia following chemotherapy. Korean J Infect Dis. 2002. 34:261–266.7. Kim YJ, Kim SI, Kim YR, Yang CW, Kang MW, Bang BK. Two successfully treated cases of posttransplant pneumonia caused by cytomegalovirus and Aspergillus coinfection. J Korean Soc Transplant. 2008. 22:130–134.8. Siu YP, Leung KT, Tong MK, Kwok YL, Wong PK, Kwan TH. Fatal case of Aspergillus coinfection in a renal transplant recipient suffering from cytomegalovirus pneumonitis. Nephrology (Carlton). 2005. 10:619–622.
Article9. Tigen E, Tigen K, Karaahmet T, Odabasi Z, Korten V. Concomitant Aspergillus and Cytomegalovirus infection in heart transplant: early diagnosis is the key to successful treatment. Exp Clin Transplant. 2009. 7:168–172.10. Leventakos K, Lewis RE, Kontoyiannis DP. Fungal infections in leukemia patients: how do we prevent and treat them? Clin Infect Dis. 2010. 50:405–415.
Article11. Balajee SA. Aspergillus terreus complex. Med Mycol. 2009. 47:Suppl 1. S42–S46.12. Cuenca-Estrella M, Bassetti M, Lass-Flörl C, Rácil Z, Richardson M, Rogers TR. Detection and investigation of invasive mould disease. J Antimicrob Chemother. 2011. 66:Suppl 1. i15–i24.
Article13. Wu CJ, Lee HC, Lo HJ, Ko WC. Resolution of galactomannan antigenemia in a patient receiving oral voriconazole for chronic necrotizing pulmonary aspergillosis. Diagn Microbiol Infect Dis. 2011. 70:528–530.
Article14. Nguyen Q, Estey E, Raad I, Rolston K, Kantarjian H, Jacobson K, Konoplev S, Ghosh S, Luna M, Tarrand J, Whimbey E. Cytomegalovirus pneumonia in adults with leukemia: an emerging problem. Clin Infect Dis. 2001. 32:539–545.
Article15. Chemaly RF, Torres HA, Hachem RY, Nogueras GM, Aguilera EA, Younes A, Luna MA, Rodriguez G, Tarrand JJ, Raad II. Cytomegalovirus pneumonia in patients with lymphoma. Cancer. 2005. 104:1213–1220.
Article16. Honda J, Yonemitsu J, Kitajima H, Yosida N, Fumirori T, Oizumi K. Clinical utility of capillary polymerase chain reaction for diagnosis of Cytomegalovirus pneumonia. Scand J infect Dis. 2001. 33:702–705.
Article17. Mori T, Kato J. Cytomegalovirus infection/disease after hematopoietic stem cell transplantation. Int J Hematol. 2010. 91:588–595.
Article18. Torres HA, Aguilera E, Safdar A, Rohatgi N, Raad II, Sepulveda C, Luna M, Kontoyiannis DP, Chemaly RF. Fatal cytomegalovirus pneumonia in patients with haematological malignancies: an autopsy-based case-control study. Clin Microbiol Infect. 2008. 14:1160–1166.
Article19. Choi SM, Lee DG, Park SH, Kim SH, Kim YJ, Min CK, Kim HJ, Lee S, Choi JH, Yoo JH, Kim DW, Lee JW, Min WS, Shin WS, Kim CC. Characteristics of cytomegalovirus diseases among hematopoietic stem cell transplant recipients : a 10-year experience at an university hospital in Korea. Infect Chemother. 2009. 41:9–19.
Article20. Avery RK, Marty FM, Strasfeld L, Lee I, Arrieta A, Chou S, Tatarowicz W, Villano S. Oral maribavir for treatment of refractory or resistant cytomegalovirus infections in transplant recipients. Transpl Infect Dis. 2010. 12:489–496.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Invasive Aspergillosis Characterized by the Formation of Large Bronchial Cast in Patient with Acute Myelogenous Leukemia
- A Case of Acute Myelogenous Leukemia during Pregnancy
- Two Successfully Treated Cases of Posttransplant Pneumonia Caused by Cytomegalovirus and Aspergillus Coinfection
- Human Cytomegalovirus Pneumonia and Pulmonary Aspergillosis in a Patient with Acute Myelogenous Leukemia following Chemotherapy
- Sweet's Syndrome with Myelodysplastic Syndrome Progressing to Acute Myelogenous Leukemia
