A Case of Congenital Adrenal Hyperplasia Combined with a Testicular Adrenal Rest Tumor and Adrenal Incidentaloma
- Affiliations
-
- 1Department of Pediatrics, Dong-A University College of Medicine.
- 2Department of Diagnostic Radiology, Dong-A University College of Medicine.
- KMID: 1523107
- DOI: http://doi.org/10.3803/jkes.2007.22.5.365
Abstract
- The fundamental defect among patients with congenital adrenal hyperplasia (CAH) due to 21-hydroxylse deficiency is the inability to synthesize cortisol and aldosterone adequately. Ineffective cortisol synthesis signals the hypothalamus and pituitary to increase the production of corticotropin releasing hormone and adrenocorticotropic hormone, respectively. Consequently, the adrenal glands become hyperplastic. It is well known that an adrenal adenoma can develop from hyperplastic tissue under increased corticotropin stimulation of the adrenal cortex in patients that are suffering with CAH. The etiologic mechanism of adrenal incidentaloma remains uncertain, but several hypotheses have been suggested. A testicular adrenal rest tumor has been reported to form in association with the excessive secretion of adrenal androgen by inadequate control after adolescence in CAH. We present a case of poorly controlled salt-losing CAH due to 21-hydroxylase deficiency combined with a testicular adrenal rest tumor and adrenal incidentaloma.
MeSH Terms
-
Adenoma
Adolescent
Adrenal Cortex
Adrenal Glands
Adrenal Hyperplasia, Congenital*
Adrenal Rest Tumor*
Adrenocorticotropic Hormone
Aldosterone
Corticotropin-Releasing Hormone
Humans
Hydrocortisone
Hypothalamus
Steroid 21-Hydroxylase
Adrenocorticotropic Hormone
Aldosterone
Corticotropin-Releasing Hormone
Hydrocortisone
Steroid 21-Hydroxylase
Figure
-

Fig. 1 Serial levels of 17-OHP. After detecting testicular adrenal rest tumor and adrenal incidnetaloma, the patient's drug compliance improved and serum 17-OHP levels was well controlled. Dotted line shows reference ranges (0.45~3.5 ng/mL).
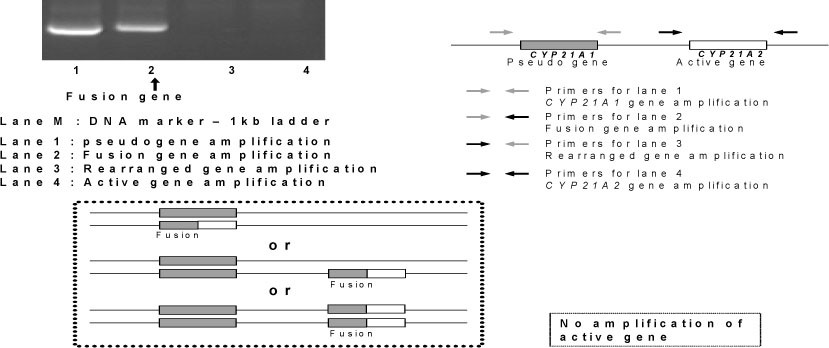
Fig. 2 Gene study of 21-hydroxylase deficiency. By allele specific PCR-sequencing method, the case shows the fusion of the 5' CYP21A2 (active gene) and 3' CYP21A1 (pseudogene). There is a complete defect to amplify no active gene at all.
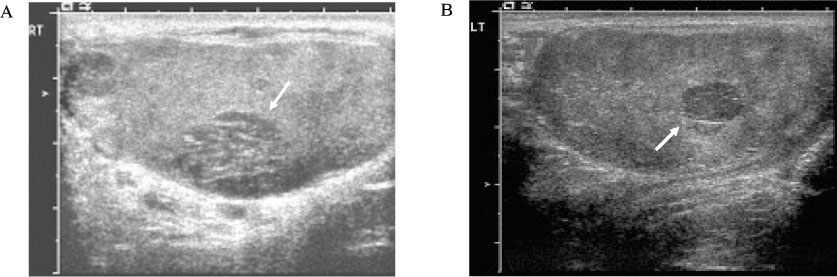
Fig. 3 Image of testicular ultrasonography. Longitudinal sonogram of the right testis shows a 1.2 × 1.6 cm sized poorly defined intratesticular mass with variable echogenicity (A). Longitudinal sonogram of the left testis shows a 0.7 × 0.8 cm sized poorly defined heterogeneous hypoechoic intratesticular mass (B).
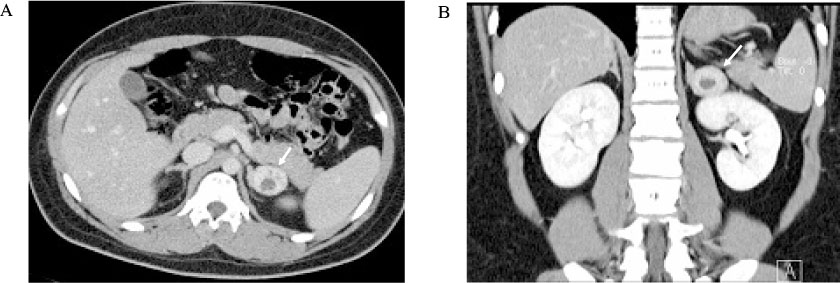
Fig. 4 Image of adrenal computed tomography. The transverse view (A) and coronal view (B) of contrast material enhanced CT scan demonstrate a 2.7 × 3.5 cm sized left adrenal incidentaloma, which is well defined ovoid enhancing mass with multiple cystic areas.
Reference
-
1. White PC, Speiser PW. Congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Endocr Rev. 2000. 21:245–291.2. White PC, Speiser PW. Long-term consequences of childhood-onset congenital adrenal hyperplasia. Best Pract Res Clin Endocrinol Metab. 2002. 12:273–288.3. Kim JM. Standard growth value in Korean children and adolescents, 2005. 2006. In : Program and Abstract, the 56th Annual Spring Meeting of the Korean Pediatric Society; 2006 April 28-29; Youngpyung. Seoul: The Korean Pediatric Society;27–41.4. Choi BG. Diagnostic criteria of obesity in Korean children and adolescents, 2005. 2006. In : Program and Abstract, the 56th Annual Spring Meeting of the Korean Pediatric Society; 2006 April 28-29; Youngpyung. Seoul: The Korean Pediatric Society;43–62.5. Lee JK, et al. Standard blood pressure value in Korean children and adolescents, 2005. 2006. In : Program and Abstract, the 56th Annual Spring Meeting of the Korean Pediatric Society; 2006 April 28-29; Youngpyung. Seoul: The Korean Pediatric Society;63–90.6. Lee H. CYP21 mutations and congenital adrenal hyperplasia. Clin Genet. 2001. 59:293–301.7. Linos DA. Adrenal incidentaloma. Hormones. 2003. 2:12–21.8. Thompson GB, Young WF Jr. Adrenal incidentaloma. Curr Opin Oncol. 2003. 15:84–90.9. Patocs A, Toth M, Barta C, Sasvari-Szekely M, Varga I, Szucs N, Jakab C, Glaz E, Racz K. Hormonal evaluation and mutation screening for steroid 21-hydroxylase deficiency in patients with unilateral and bilateral adrenal incidentalomas. Eur J Endocrinol. 2002. 147:349–355.10. Jaresch S, Kornely E, Kley HK, Schlaghecke R. Adrenal incidentalomas and patients with homozygous or heterozygous congenital adrenal hyperplasia. J Clin Endocrinol Metab. 1992. 74:685–689.11. Wang J, Bissada MA, Williamson HO, Yakout H, Bissada NK. Adrenal tumors associated with inadequately treated congenital adrenal hyperplasia. Can J Urol. 2002. 9:563–1564.12. Harinarayana CV, Renu G, Ammini AC, Khurana ML, Ved P, Karmarkar MG, Ahuja MM, Berry M. Computed tomography in untreated congenital adrenal hyperplasia. Pediatr Radiol. 1991. 21:103–105.13. Young WF Jr. Management approaches to adrenal incidentalomas. Endocrinol Metab Clin North Am. 2000. 29:159–185.14. Kim HY, Kim SG, Lee KW, Seo JA, Kim NH, Choi KM, Baik SH, Choi DS. Clinical study of adrenal incidentaloma in Korea. Korean J Intern Med. 2005. 20:303–309.15. Wilkins L, Fleishmann W, Howard JE. Macrogenitosomia precox associated with hyperplasia of the androgenic tissue of the adrenal and death from corticoadrenal insufficiency. Endocrinology. 1940. 26:385–395.16. Stikkelbroeck NM, Otten BJ, Pasic A, Jager GJ, Sweep CG, Noordam K, Hermus AR. High prevalence of testicular adrenal rest tumors, impaired spermatogenesis, and Leydig cell failure in adolescent and adult males with congenital adrenal hyperplasia. J Clin Endocrinol Metab. 2001. 86:5721–5728.17. Avila NA, Shawker TS, Jones JV, Cutler GB Jr, Merke DP. Testicular adrenal rest tissue in congenital adrenal hyperplasia: serial sonographic clinical findings. AJR Am J Roentgenol. 1999. 172:1235–1238.18. Dogra V, Nathan J, Bhatt S. Sonographic appearance of testicular adrenal rest tissue in congenital adrenal hyperplasia. J Ultrasound Med. 2004. 23:979–981.19. Nagamine WH, Mehta SV, Vade A. Testicular adrenal rest tumors in a patient with congenital adrenal hyperplasia: onographic and magnetic resonance imaging findings. J ultrasound Med. 2005. 24:1717–1720.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of testicular adrenal rest tumor in a male child with congenital adrenal hyperplasia
- Ultrasound Follow-Up of Testicular Adrenal Rest Tumors with Congenital Adrenal Hyperplasia: Report of Three Cases
- Testicular Adrenal Rest Tumor in 11-Beta-Hydroxylase Deficiency Driven Congenital Adrenal Hyperplasia
- A Case of Congenital Adrenal Hyperlasia Misdiagnosed as Leydig Cell Tumor
- A Case of Congenital Lipoid Adrenal Hyperplasia: Early Diagnosis by Using Computed Tomography
