A Case of Pituitary Metastasis of Breast Cancer Presenting as Diabetes Insipidus and Panhypopituitarism
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea College of Medicine, Korea.
- KMID: 1523093
- DOI: http://doi.org/10.3803/jkes.2007.22.2.125
Abstract
- Metastasis to the pituitary gland from systemic cancer is a rare condition. The breast and lung are the most common sites of primary tumor metastasis. Pituitary metastasis may present with diabetes insipidus, cranial nerve palsy and hypopituitarism, and diabetes insipidus is the most frequent symptom at presentation. We report here on a 44 year-old woman with pituitary metastasis from breast cancer, and she developed central diabetes insipidus and hypopituitarism. The clinical diagnosis was made by performing a water deprivation test, a combined pituitary test and a MRI brain scan, and the latter showed metastatic tumor in the pituitary gland with invasion of the pituitary stalk. Symptomatic relief was obtained with administration of desmopressin; the urine osmolarity was increased with this treatment. We report here on a case of pituitary metastasis from breast cancer and the patient developed central diabetes insipidus and hypopituitarism. We also include a review of the relevant literature.
MeSH Terms
-
Adult
Brain
Breast Neoplasms*
Breast*
Cranial Nerve Diseases
Deamino Arginine Vasopressin
Diabetes Insipidus*
Diabetes Insipidus, Neurogenic
Diagnosis
Female
Humans
Hypopituitarism
Lung
Magnetic Resonance Imaging
Neoplasm Metastasis*
Osmolar Concentration
Pituitary Gland
Water Deprivation
Deamino Arginine Vasopressin
Figure
-
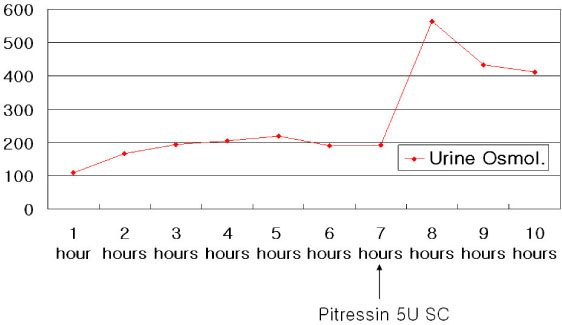
Fig. 1 Water deprivation test.
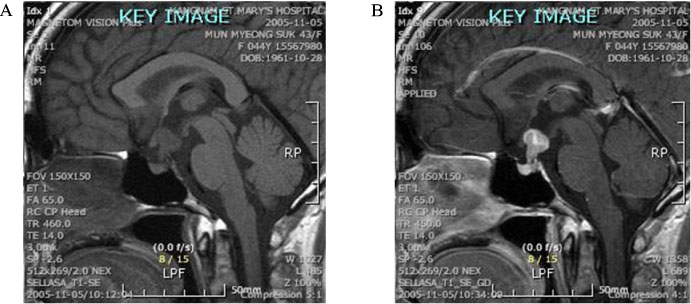
Fig. 2A, 2B 1.5 × 1.3 × 1.3 cm sized homogenous lobulated low signal intensity mass is noted on nonenhanced sagittal T1WI in pituitary stalk and suprasellar cistern, which shows heterogenous enhancement on gadolinum enhanced image.
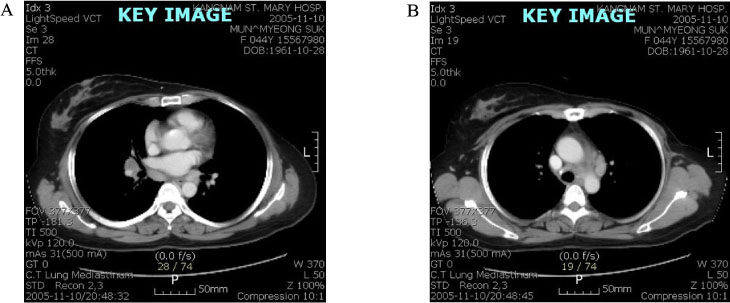
Fig. 3A, 3B On contrast enhanced chest CT, left breast is not visualized and conglomerated nodules with decreased attenuation are noted in left paratracheal mediastinum and right hilum.

Fig. 4A, 4B, 4C On axial FLAIR and T2WI images, asymmetric two high signal intensity nodules are noted in left frontal lobe, suggesting brain metastasis. On coronal T1WI with enhancement, focal enhanced ovoid lesion is noted in right scalp representing scalp metastasis.
Cited by 1 articles
-
A Case of Pituitary Metastasis from Breast Cancer That Presented as Left Visual Disturbance
Young Ha Kim, Beom jun Lee, Kyung Jin Lee, Jin Hee Cho
J Korean Neurosurg Soc. 2012;51(2):94-97. doi: 10.3340/jkns.2012.51.2.94.
Reference
-
1. Weil RJ. Pituitary metastasis. Arch Neurol. 2002. 59:1962–1963.2. Komninos J, Vlassopoulou V, Protopapa D, Korfias S, Kontogeorgos G, Sakas DE, Thalassinos NC. Tumors metastatic to the pituitary gland: case report and literature review. J Clin Endocrinol Metab. 2004. 89:574–580.3. Kim HC, Lee HJ. A Clinical study of sellar and parasellar lesions. J Kor Neurosurg Soc. 1973. 2:37–49.4. Jung SW, Lee KW, Kang MS, Ahn JH, Kim BS, Kim MC. Metastatic renal cell carcinoma to the hypophysis. J Kor Med Assoc. 1991. 34:671–677.5. Shin ET, Lee EJ, Kim KR, Lee KM, Bae HD, Lee KS, Chung YS, Ahn KJ, Lim SK, Lee HC, Huh KB. A Case of pituitary metastasis from periampullary carcinoma. J Kor Endocrinol. 1993. 8:88–93.6. Lee SH, Song YD, Kim HS, Lee YM, Yoon YS, Lim SK, Nam JH, Kwon SH, Kim KR, Lee HC, Huh KB. A Case of central diabetes insipidus caused by metastatic malignant lymphoma. J Kor Endocrinol Soc. 1997. 12:596–601.7. Ruelle A, Palladino M, Andrioli GC. Pituitary metastases as presenting lesions of malignancy. J Neurosurg Sci. 1992. 36:51–54.8. Morita A, Meyer FB, Laws ER Jr. Symptomatic pituitary metastases. J Neurosurg. 1998. 89:69–73.9. Sioutos P, Yen V, Arbit E. Pituitary gland metastases. Ann Surg Oncol. 1996. 3:94–99.10. McCormick PC, Post KD, Kandji AD, Hays AP. Metastatic carcinoma to the pituitary gland. Br J Neurosurg. 1989. 3:71–79.11. Max MB, Deck MD, Rottenberg DA. Pituitary metastasis: incidence in cancer patients and clinical differentiation from pituitary adenoma. Neurology. 1981. 31:998–1002.12. Houck WA, Olson KB, Horton J. Clinical features of tumor metastasis to the pituitary. Cancer. 1970. 26:656–659.13. Teears RJ, Silverman EM. Clinicopathologic review of 88 cases of carcinoma etastatic to the putuitary gland. Cancer. 1975. 36:216–220.14. Branch CL Jr, Laws ER Jr. Metastatic tumors of the sella turcica masquerading as primary pituitary tumors. J Clin Endocrinol Metab. 1987. 65:469–474.15. Delattre JY, Castelain C, Davila L, Schadeck B, Poisson M. Metastasis to the pituitary stalk in a case of breast cancer. Rev Neurol (Paris). 1990. 146:455–456.16. Chiang MF, Brock M, Patt S. Pituitary metastases. Neurochirurgia (Stuttg). 1990. 33:127–131.17. Leramo OB, Booth JD, Zinman B, Bergeron C, Sima AA. Morley TPL Hyperprolactinemia, hypopituitarism, and chiasmal compression due to carcinoma metastatic to the pituitary. Neurosurgery. 1981. 8:477–480.18. Schubiger O, Haller D. Metastases to the pituitary-hypothalamic axis. An MR study of 7 symptomatic patients. Neuroradiology. 1992. 34:131–134.19. Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am. 1999. 28:99–100.20. Chaudhuri R, Twelves C, Cox TC, Bingham JB. MRI in diabetes insipidus due to metastatic breast carcinoma. Clin Radiol. 1992. 46:184–188.21. Moses AM, Clayton B, Hochhauser L. Use of T1-weighted MR imaging to differentiate between primary polydipsia and central diabetes insipidus. Am J Neuroradiol. 1992. 13:1273–1277.22. Nelson PB, Robinson AG, Martinez AJ. Metastatic tumor of the pituitary gland. Neurosurgery. 1987. 21:941–944.23. Yap HY, Tashima CK, Blumenschein GR, Eckles N. Diabetes insipidus and breast cancer. Arch Intern Med. 1979. 139:1009–1011.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Solitary Pituitary Metastasis of Advanced Breast Cancer Treated with Anti-Human Epidermal Growth Factor Receptor 2 Drug
- Primary Granulomatous Hypophysitis Presenting with Panhypopituitarism and Central Diabetes Insipidus
- A Case of Pituitary Metastasis of Lung Presenting as Diabetes Insipidus
- A case of Sheehan's syndrome with central diabetes insipidus showing hemorrhagic pituitary apoplexy
- A Case of Pituitary Metastasis from Breast Cancer That Presented as Left Visual Disturbance
