A Case of Pituitary Metastasis from Breast Cancer That Presented as Left Visual Disturbance
- Affiliations
-
- 1Department of Otolaryngology-HNS, College of Medicine, The Catholic University of Korea, Seoul, Korea. entcho@catholic.ac.kr
- 2Department of Neurosurgery, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 1441417
- DOI: http://doi.org/10.3340/jkns.2012.51.2.94
Abstract
- Tumors that metastasize to the pituitary gland are unusual, and are typically seen in elderly patients with diffuse malignant disease. The most common metastases to the pituitary are from primary breast and lung cancers. We report a 65-year-old woman with pituitary metastasis from breast cancer who presented with recent-onset left progressive deterioration of visual acuity and visual field. The clinical diagnosis was made after brain and sellar magnetic resonance imaging showed a large sellar mass compressing the optic chiasm and invading the pituitary stalk. An otorhinolaryngology and neurosurgery team removed the tumor via a transsphenoidal approach, and this procedure obtained symptomatic relief. Postoperatively, metastasis from breast invasive ductal adenocarcinoma was confirmed histologically. We report this unusual case with a review of the relevant literature.
MeSH Terms
Figure
-
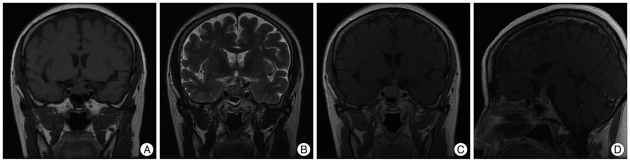
Fig. 1 Preoperative coronal view of T1 weighted image of sellar MRI (A), coronal view of T2 weighted image (B), coronal view of T1 Gadolinum enhanced image (C), sagittal view of T1 Gadolinum enhanced image (D). Images show the dumbbell shape pituitary mass with T1 intermediate, T2 intermediate and well enhancing nature, compressing the optic chiasm and invading the pituitary stalk.
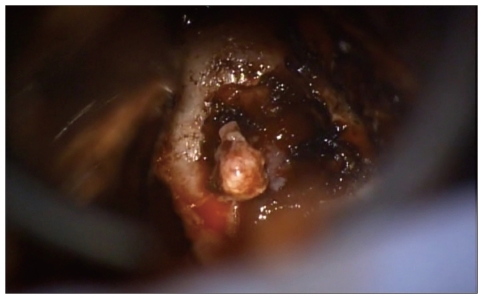
Fig. 2 Pituitary mass during the operation. The contents and colors were just similar with pituitary adenoma.
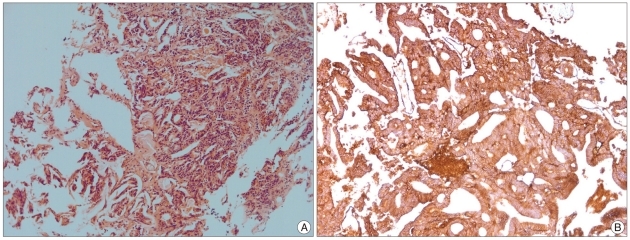
Fig. 3 Microscopic finding (HE, ×100). Characteristic findings of adenocarcinoma consist with invasive proliferation of cancer cell foci, formation of ductal structures by cancer cells were seen (A), immunohistochemical staining with MOC-31, which is a marker for adenocarcinoma showed positive (B).
Cited by 1 articles
-
Differential Diagnosis and Management of a Pituitary Mass with Renal Cell Carcinoma
Joo Min Hwang, Yong Hwy Kim, Tae Min Kim, Sung Hye Park
J Korean Neurosurg Soc. 2013;54(2):132-135. doi: 10.3340/jkns.2013.54.2.132.
Reference
-
1. Chiang MF, Brock M, Patt S. Pituitary metastases. Neurochirurgia (Stuttg). 1990; 33:127–131. PMID: 2203980.
Article2. Fassett DR, Couldwell WT. Metastases to the pituitary gland. Neurosurg Focus. 2004; 16:E8. PMID: 15191337.
Article3. Heshmati HM, Scheithauer BW, Young WF. Metastases to the pituitary gland. Endocrinologist. 2002; 12:45–49.
Article4. Houck WA, Olson KB, Horton J. Clinical features of tumor metastasis to the pituitary. Cancer. 1970; 26:656–659. PMID: 5272295.
Article5. Komninos J, Vlassopoulou V, Protopapa D, Korfias S, Kontogeorgos G, Sakas DE, et al. Tumors metastatic to the pituitary gland : case report and literature review. J Clin Endocrinol Metab. 2004; 89:574–580. PMID: 14764764.
Article6. Kurkjian C, Armor JF, Kamble R, Ozer H, Kharfan-Dabaja MA. Symptomatic metastases to the pituitary infundibulum resulting from primary breast cancer. Int J Clin Oncol. 2005; 10:191–194. PMID: 15990968.
Article7. Kwak JW, Jie BS, Hong SH, Kim JH, Lee SH, Jo JH, et al. A case of pituitary metastasis of breast cancer presenting as diabetes insipidus and panhypopituitarism. J Korean Endocr Soc. 2007; 22:125–129.
Article8. Morita A, Meyer FB, Laws ER Jr. Symptomatic pituitary metastases. J Neurosurg. 1998; 89:69–73. PMID: 9647174.
Article9. Moses AM, Clayton B, Hochhauser L. Use of T1-weighted MR imaging to differentiate between primary polydipsia and central diabetes insipidus. AJNR Am J Neuroradiol. 1992; 13:1273–1277. PMID: 1414815.10. Ruelle A, Palladino M, Andrioli GC. Pituitary metastases as presenting lesions of malignancy. J Neurosurg Sci. 1992; 36:51–54. PMID: 1323647.11. Shin ET, Lee EJ, Kim KR, Lee KM, Bae HD, Lee KS, et al. A case of pituitary metastasis from periampullary carcinoma. J Korean Soc Endocrinol. 1993; 8:88–93.12. Sioutos P, Yen V, Arbit E. Pituitary gland metastases. Ann Surg Oncol. 1996; 3:94–99. PMID: 8770309.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Solitary Pituitary Metastasis of Advanced Breast Cancer Treated with Anti-Human Epidermal Growth Factor Receptor 2 Drug
- A Case of Compressive Optic Neuropathy due to Breast Cancer Metastasis
- A Case of Pituitary Metastasis of Breast Cancer Presenting as Diabetes Insipidus and Panhypopituitarism
- A Case of Unusual Pituitary Apoplexy Presented as Aseptic Meningitis
- Extensive Pituitary Apoplexy after Chemotherapy in a Patient with Metastatic Breast Cancer
