Neovascularization in Outer Membrane of Chronic Subdural Hematoma : A Rationale for Middle Meningeal Artery Embolization
- Affiliations
-
- 1Department of Molecular Medicine and Biopharmaceutical Sciences, Graduate School of Convergence Science and Technology, College of Medicine or College of Pharmacy, Seoul National University, Seoul, Korea
- 2Department of Nuclear Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 3Department of Pathology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 4Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 5Radiation Medicine Institute, Seoul National University College of Medicine, Seoul, Korea
- 6Institute on Aging, Seoul National University, Seoul, Korea
- KMID: 2553120
- DOI: http://doi.org/10.3340/jkns.2023.0105
Abstract
Objective
: Chronic subdural hematomas (cSDHs) are generally known to result from traumatic tears of bridging veins. However, the causes of repeat spontaneous cSDHs are still unclear. We investigated the changes in vasculature in the human dura mater and outer membrane (OM) of cSDHs to elucidate the cause of their spontaneous repetition.
Methods
: The dura mater was obtained from a normal control participant and a patient with repeat spontaneous cSDHs. The pathological samples from the patient included the dura mater and OM tightly adhered to the inner dura. The samples were analyzed with a particular focus on blood and lymphatic vessels by immunohistochemistry, 3-dimensional imaging using a transparent tissue clearing technique, and electron microscopy.
Results
: The dural border cell (DBC) layer of the dura mater and OM were histologically indistinguishable. There were 5.9 times more blood vessels per unit volume of tissue in the DBC layer and OM in the patient than in the normal control. The DBC layer and OM contained pathological sinusoidal capillaries not observed in the normal tissue; these capillaries were connected to the middle meningeal arteries via penetrating arteries. In addition, marked lymphangiogenesis in the periosteal and meningeal layers was observed in the patient with cSDHs.
Conclusion
: Neovascularization in the OM seemed to originate from the DBC layer; this is a potential cause of repeat spontaneous cSDHs. Embolization of the meningeal arteries to interrupt the blood supply to pathological capillaries via penetrating arteries may be an effective treatment option.
Keyword
Figure
-
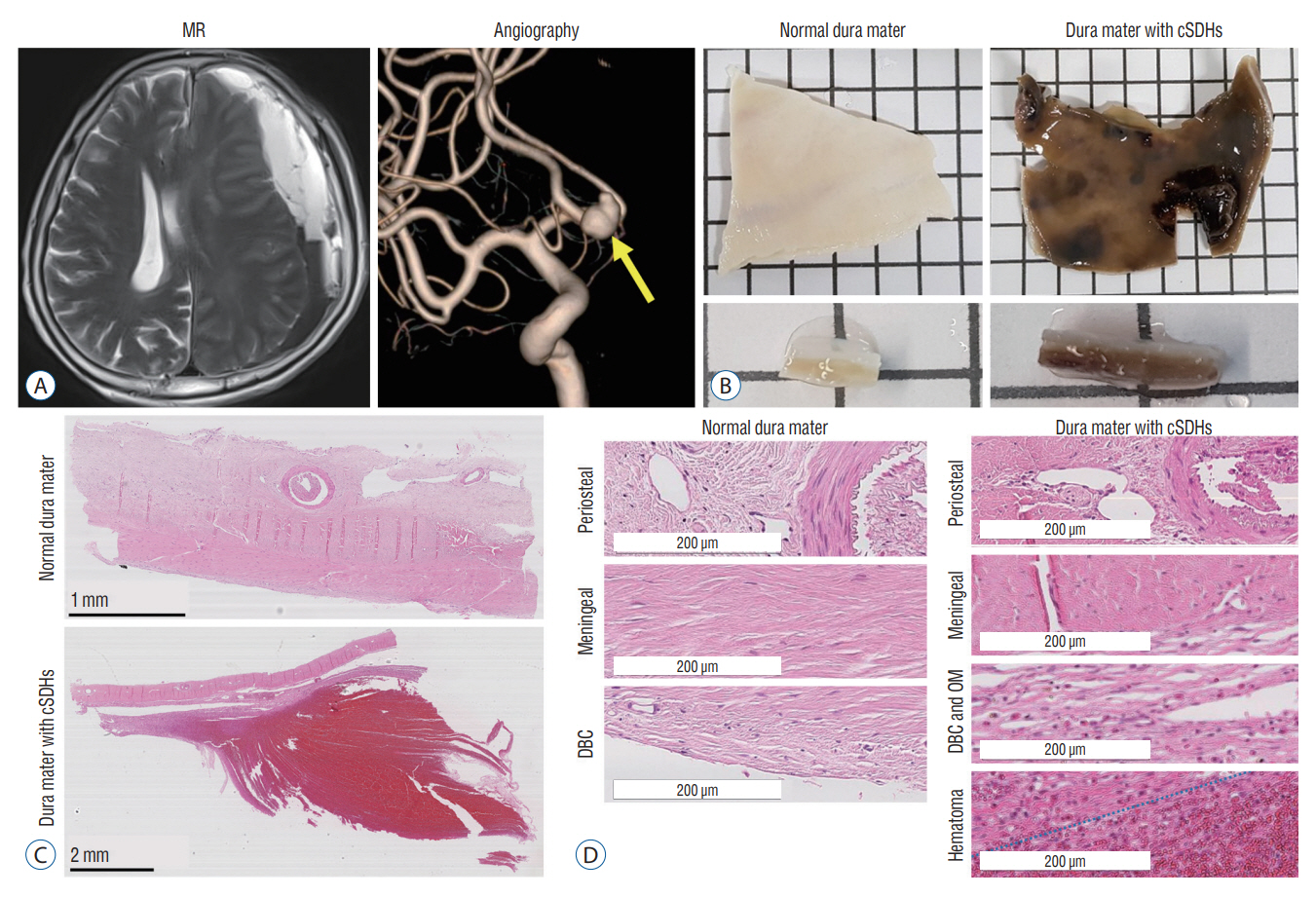
Fig. 1. Imaging and histologic data. A : MR and 3-dimensional reconstructive angiographic images of a patient with repeat spontaneous cSDHs. The patient underwent clipping of the unruptured intracranial aneurysm at the anterior communicating artery (yellow arrow, right) and removal of cSDHs with adjacent dura mater and OM (left) simultaneously via left-sided frontotemporal craniotomy. B : Gross photos of the normal control and pathologic dura mater attached to the OM of cSDHs. C and D : Representative Hematoxylin & eosin staining images of the dura mater from the normal control and patient with cSDHs. Scale bar : 1 mm, normal dura mater; 2 mm, dura mater with cSDHs. D : In the high magnification images, the DBC layer and OM of cSDHs showed looser connective tissue and numerous cavities than the DBC layer in the normal control. The blue line indicates the boundary between the OM and hematoma. Scale bar, 200 µm. MR : magnetic resonance, cSDH : chronic subdural hematoma, DBC : dural border cell, OM : outer membrane.
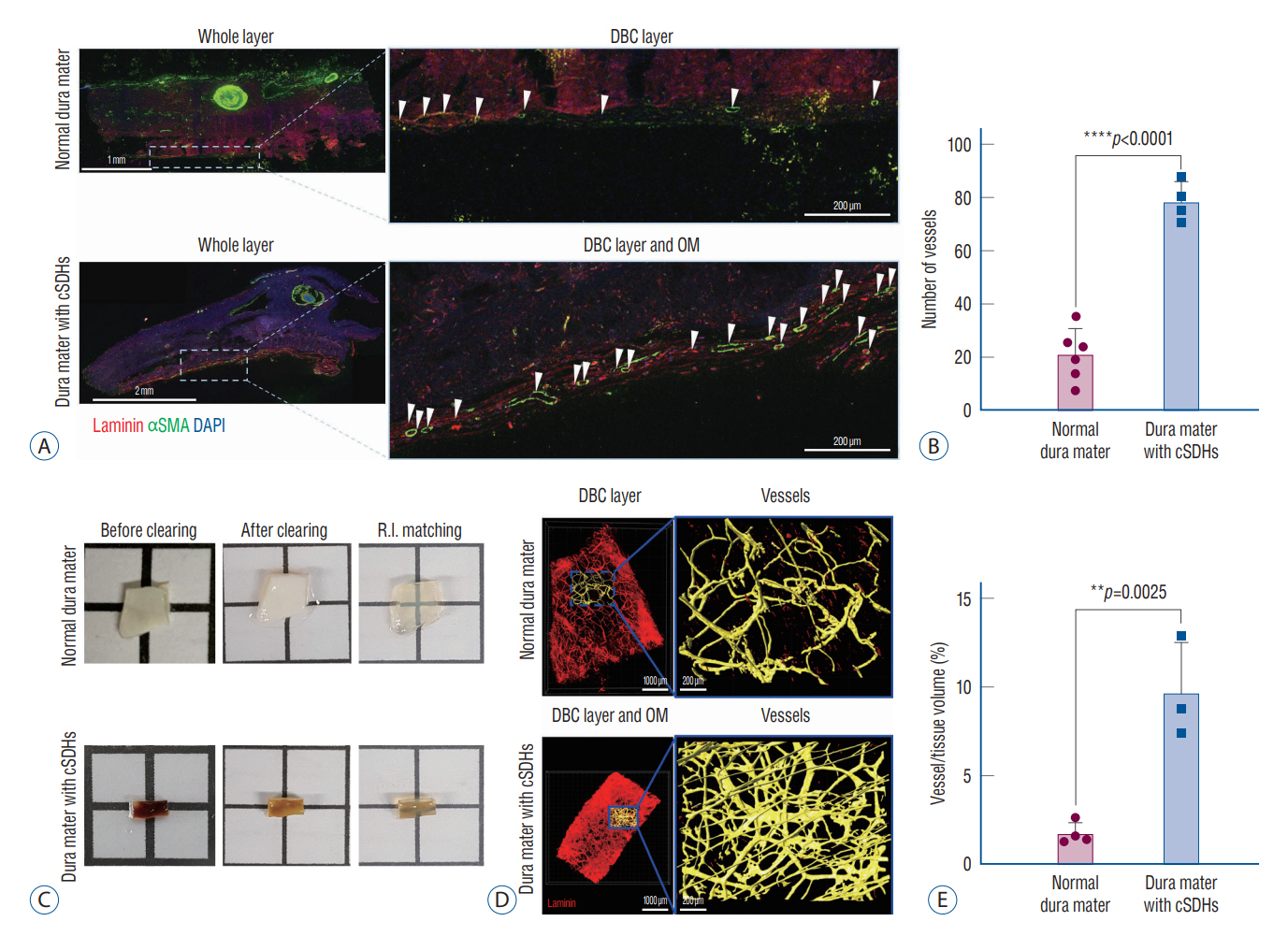
Fig. 2. Neovascularization in the DBC layer of the dura mater and OM of cSDHs. A : Representative images of vessels immunolabeled with laminin (red) and αSMA (green) in the dura mater of the normal control (scale bar, 1 mm) and patient with cSDHs (scale bar, 2 mm). There was a greater increase in vessels in the DBC layer and OM of cSDHs compared to the normal control. White arrowheads indicate vessels. Scale bar, 200 μm. B : Quantification of the number of vessels per area (mm2) of the DBC layer. Each dot represents the number of vessels from 4–6 sections in the dura mater. Data are presented as the average±SD. C : Schematic of the procedure for preparing transparent tissue samples. After clearing, the images showed the removal of lipids from the polymerized tissue. Refractive index (R.I.)-matched tissues were transparent. D : Representative images of the 3D vasculature stained with laminin in the normal control and DBC layer and OM of cSDHs in the patient. Scale bar, 1 mm. The vessels in the volume-rendered images are shown in yellow at 5X magnification (scale bar, 200 μm). E : Quantification of the vascular volume per tissue volume (μm3). The total volume of vessels was higher in the specimen from the patient with cSDHs than in that from the normal control. Data are presented as the average±SD (**p<0.005, ****p<0.0001). DBC : dural border cell, cSDH : chronic subdural hematoma, OM : outer membrane, αSMA : α-smooth muscle actin, DAPI : 4′,6-diamidino2-phenylindole, SD : standard deviation.
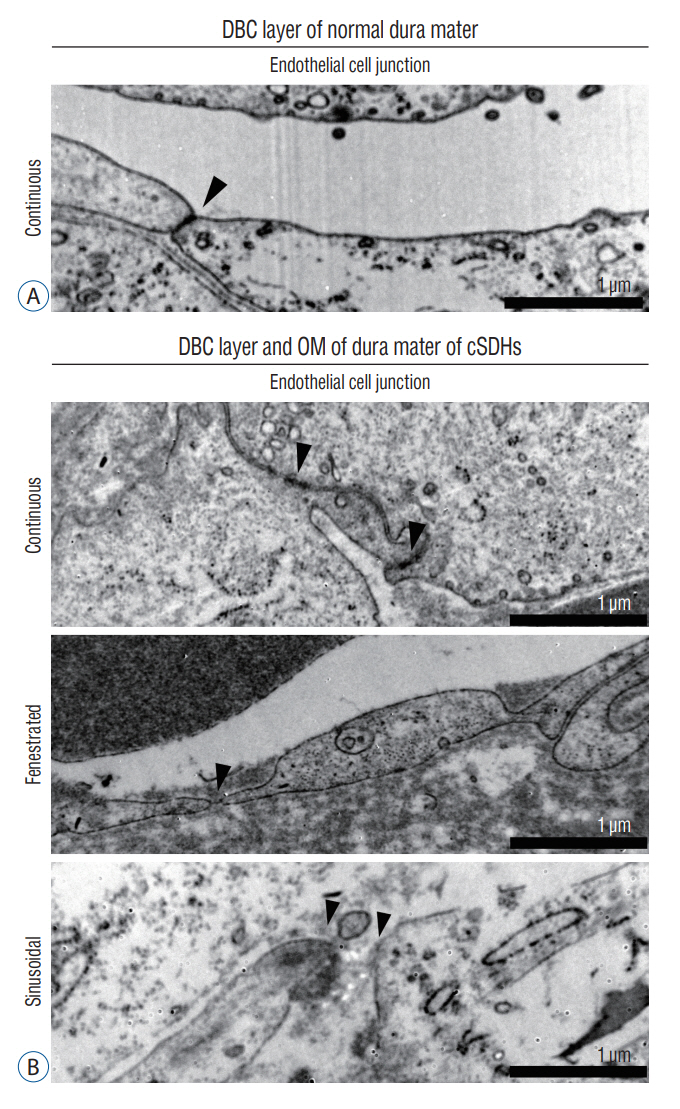
Fig. 3. Types of capillaries in the DBC layer of the dura mater and OM of cSDHs. A : Representative TEM image of a continuous capillary in the DBC layer of the normal control. Scale bar, 1 μm. B : Representative TEM images of the capillary type in the DBC layer of the dura mater and OM of cSDHs from the patient. Black arrowheads indicate tight junctions in a continuous capillary, a pore with a diaphragm in a fenestrated capillary, and gaps without junctions and diaphragms in a sinusoidal capillary. Scale bar, 1 μm. DBC : dural border cell, OM : outer membrane, cSDH : chronic subdural hematoma, TEM : transmission electron microscopy.
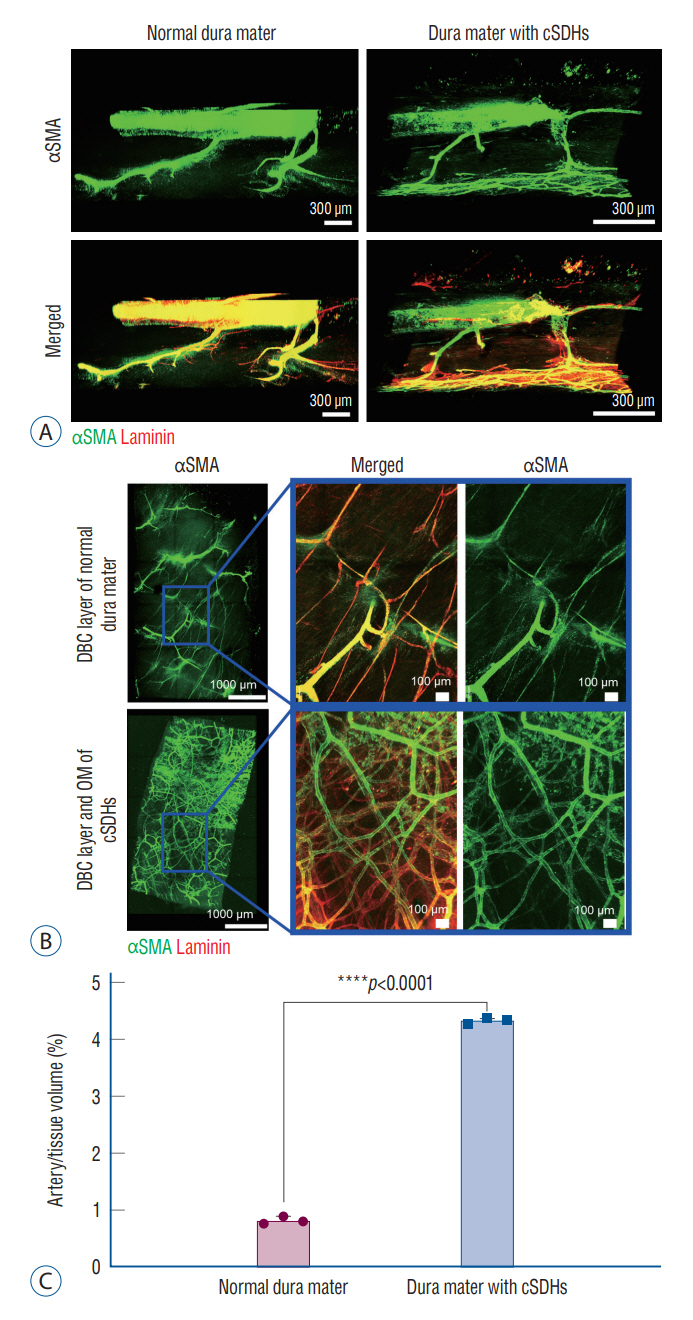
Fig. 4. Connection between MMAs and newly formed capillaries in the DBC layer and OM of cSDHs. A : Representative images of 3-dimensional (3D) vessels stained with laminin (red) and αSMA (green) in the entire dura mater from the periosteal to the DBC layers. The penetrating arteries connected to the MMAs in the periosteal layer and the capillaries in the DBC layer. A significant increase in capillaries in the DBC layer and OM of cSDHs was observed. Scale bar, 300 μm. B : Laminin (red)- and αSMA (green)-labeled arteries are shown after volume rendering steps. The 3D volume of the capillaries in the DBC dural layer and OM of cSDHs is shown in yellow. C : Quantification of the arterial volume (μm3) in the DBC layer and OM. The volume of capillaries increased significantly. Data are presented as the average±standard deviation (****p<0.0001). cSDH : chronic subdural hematoma, αSMA : α-smooth muscle actin, DBC : dural border cell, OM : outer membrane, MMA : middle meningeal artery.

Fig. 5. The formation of lymphatic vessels. The white and yellow arrowheads indicate the loops and sprouts of lymphatic vessels, respectively. A : Representative images of immunostaining of vessels (laminin, red) and lymphatic vessels (PDPN, green) in the periosteal and meningeal layers of four pieces of tissue. B : Representative magnified images of loops and sprouts in lymphatic vessels. C and D : Quantification of the number of loops and sprouts per area (μm3) in the dura mater. Greater formation of loops and sprouts was observed in the patient with cSDHs than in the normal control. Data are presented as the average±standard deviation (*p<0.05). PDPN : podoplanin, cSDH : chronic subdural hematoma, ns : not significant.
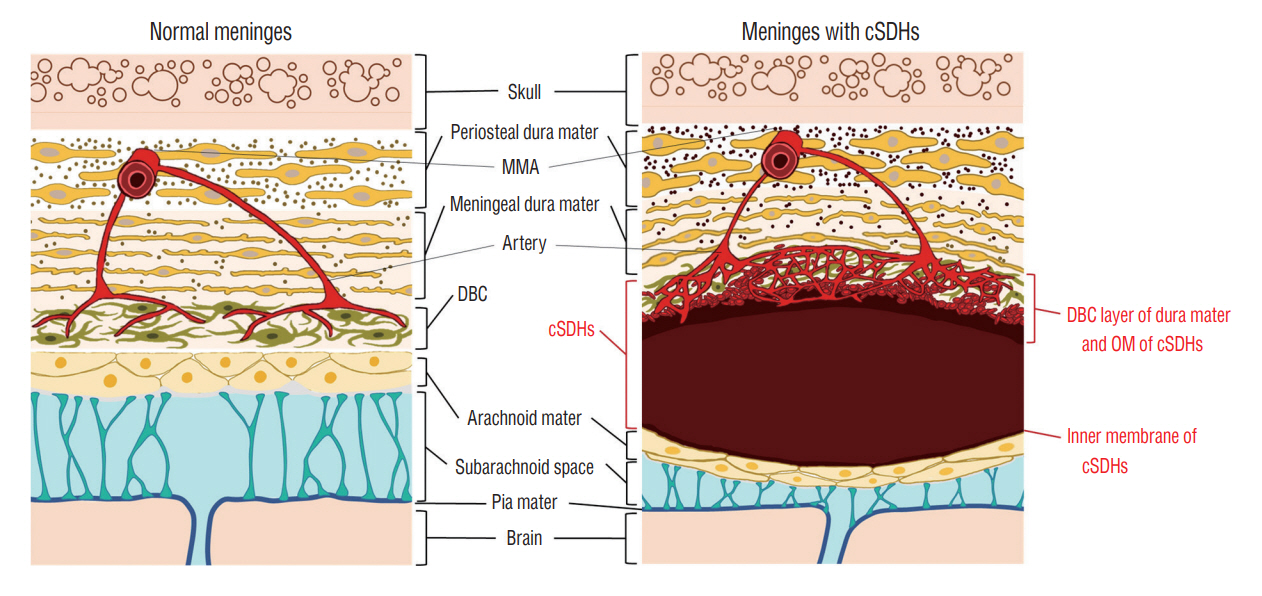
Fig. 6. Illustration of the pathological characteristics of the dura mater and cSDHs. As the hematoma accumulates in the subdural space, membranes envelop the cSDHs. Compared to the inner membrane of cSDHs, the OM of cSDHs seems to originate from the DBC layer of the dura mater based on the histologically indistinguishable plane between the DBC layer and OM. The number of vessels in the DBC layer and OM in the patient with cSDHs was much higher than that in the DBC layer of the normal control. Newly formed vessels are composed of sinusoidal capillaries, which are thought to be a probable cause of repeat spontaneous bleeding because they are fragile and present in only the pathological DBC dural layer and OM of cSDHs. Such neovessels connect to surface MMAs via penetrating arteries. Therefore, MMA embolization is a potentially effective way to block the blood supply to pathological membranes. cSDH : chronic subdural hematoma, MMA : middle meningeal artery, DBC : dural border cell, OM : outer membrane.

Reference
-
References
1. Augustin HG, Koh GY. Organotypic vasculature: from descriptive heterogeneity to functional pathophysiology. Science. 357:eaal2379. 2017.2. Ban SP, Hwang G, Byoun HS, Kim T, Lee SU, Bang JS, et al. Middle meningeal artery embolization for chronic subdural hematoma. Radiology. 286:992–999. 2018.3. Blanco R, Gerhardt H. VEGF and Notch in tip and stalk cell selection. Cold Spring Harb Perspect Med. 3:a006569. 2013.4. Bolte AC, Dutta AB, Hurt ME, Smirnov I, Kovacs MA, McKee CA, et al. Meningeal lymphatic dysfunction exacerbates traumatic brain injury pathogenesis. Nat Commun. 11:4524. 2020.5. Chen JC, Levy ML. Causes, epidemiology, and risk factors of chronic subdural hematoma. Neurosurg Clin N Am. 11:399–406. 2000.6. Cho WS, Batchuluun B, Lee SJ, Kang HS, Kim JE. Recurrent subdural hematoma from a pseudoaneurysm at the cortical branch of the middle cerebral artery after mild head injury: case report. Neurol Med Chir (Tokyo). 51:217–221. 2011.7. Edlmann E, Giorgi-Coll S, Whitfield PC, Carpenter KLH, Hutchinson PJ. Pathophysiology of chronic subdural haematoma: inflammation, angiogenesis and implications for pharmacotherapy. J Neuroinflammation. 14:108. 2017.8. Fiorella D, Arthur AS. Middle meningeal artery embolization for the management of chronic subdural hematoma. J Neurointerv Surg. 11:912–915. 2019.9. Gardner WJ. Traumatic subdural hematoma: with particular reference to the latent interval. AMA Arch Neurol Psychiatry. 27:847–858. 1932.10. Haldrup M, Ketharanathan B, Debrabant B, Schwartz OS, Mikkelsen R, Fugleholm K, et al. Embolization of the middle meningeal artery in patients with chronic subdural hematoma-a systematic review and metaanalysis. Acta Neurochir (Wien). 162:777–784. 2020.11. Hirashima Y, Kurimoto M, Nagai S, Hori E, Origasa H, Endo S. Effect of platelet-activating factor receptor antagonist, etizolam, on resolution of chronic subdural hematoma--a prospective study to investigate use as conservative therapy. Neurol Med Chir (Tokyo). 45:621–626. discussion 626. 2005.12. Ito H, Yamamoto S, Komai T, Mizukoshi H. Role of local hyperfibrinolysis in the etiology of chronic subdural hematoma. J Neurosurg. 45:26–31. 1976.13. Kageyama H, Toyooka T, Tsuzuki N, Oka K. Nonsurgical treatment of chronic subdural hematoma with tranexamic acid. J Neurosurg. 119:332–337. 2013.14. Kawakami Y, Chikama M, Tamiya T, Shimamura Y. Coagulation and fibrinolysis in chronic subdural hematoma. Neurosurgery. 25:25–29. 1989.15. Koh BI, Lee HJ, Kwak PA, Yang MJ, Kim JH, Kim HS, et al. VEGFR2 signaling drives meningeal vascular regeneration upon head injury. Nat Commun. 11:3866. 2020.16. Link TW, Boddu S, Paine SM, Kamel H, Knopman J. Middle meningeal artery embolization for chronic subdural hematoma: a series of 60 cases. Neurosurgery. 85:801–807. 2019.17. Liu X, Gao C, Yuan J, Xiang T, Gong Z, Luo H, et al. Subdural haematomas drain into the extracranial lymphatic system through the meningeal lymphatic vessels. Acta Neuropathol Commun. 8:16. 2020.18. Louveau A, Smirnov I, Keyes TJ, Eccles JD, Rouhani SJ, Peske JD, et al. Structural and functional features of central nervous system lymphatic vessels. Nature. 523:337–341. 2015.19. Mehta V, Harward SC, Sankey EW, Nayar G, Codd PJ. Evidence based diagnosis and management of chronic subdural hematoma: a review of the literature. J Clin Neurosci. 50:7–15. 2018.20. Ohba S, Kinoshita Y, Nakagawa T, Murakami H. The risk factors for recurrence of chronic subdural hematoma. Neurosurg Rev. 36:145–149. discussion 149-150. 2013.21. Parlato C, Guarracino A, Moraci A. Spontaneous resolution of chronic subdural hematoma. Surg Neurol. 53:312–315. discussion 315-317. 2000.22. Rambaud C. Bridging veins and autopsy findings in abusive head trauma. Pediatr Radiol. 45:1126–1131. 2015.23. Rauhala M, Luoto TM, Huhtala H, Iverson GL, Niskakangas T, Öhman J, et al. The incidence of chronic subdural hematomas from 1990 to 2015 in a defined Finnish population. J Neurosurg. 132:1147–1157. 2019.24. Sahyouni R, Goshtasbi K, Mahmoodi A, Tran DK, Chen JW. Chronic subdural hematoma: a perspective on subdural membranes and dementia. World Neurosurg. 108:954–958. 2017.25. Shapiro M, Walker M, Carroll KT, Levitt MR, Raz E, Nossek E, et al. Neuroanatomy of cranial dural vessels: implications for subdural hematoma embolization. J Neurointerv Surg. 13:471–477. 2021.26. Shim YS, Park CO, Hyun DK, Park HC, Yoon SH. What are the causative factors for a slow, progressive enlargement of a chronic subdural hematoma? Yonsei Med J. 48:210–217. 2007.27. Sim YW, Min KS, Lee MS, Kim YG, Kim DH. Recent changes in risk factors of chronic subdural hematoma. J Korean Neurosurg Soc. 52:234–239. 2012.28. Srivatsan A, Mohanty A, Nascimento FA, Hafeez MU, Srinivasan VM, Thomas A, et al. Middle meningeal artery embolization for chronic subdural hematoma: meta-analysis and systematic review. World Neurosurg. 122:613–619. 2019.29. Stanisic M, Aasen AO, Pripp AH, Lindegaard KF, Ramm-Pettersen J, Lyngstadaas SP, et al. Local and systemic pro-inflammatory and antiinflammatory cytokine patterns in patients with chronic subdural hematoma: a prospective study. Inflamm Res. 61:845–852. 2012.30. Wang D, Gao C, Xu X, Chen T, Tian Y, Wei H, et al. Treatment of chronic subdural hematoma with atorvastatin combined with low-dose dexamethasone: phase II randomized proof-of-concept clinical trial. J Neurosurg. 134:235–243. 2020.31. Weigel R, Hohenstein A, Schlickum L, Weiss C, Schilling L. Angiotensin converting enzyme inhibition for arterial hypertension reduces the risk of recurrence in patients with chronic subdural hematoma possibly by an antiangiogenic mechanism. Neurosurgery. 61:788–792. discussion 792-793. 2007.32. Weigel R, Schilling L, Schmiedek P. Specific pattern of growth factor distribution in chronic subdural hematoma (CSH): evidence for an angiogenic disease. Acta Neurochir (Wien). 143:811–818. discussion 819. 2001.33. Yamashima T, Yamamoto S, Friede RL. The role of endothelial gap junctions in the enlargement of chronic subdural hematomas. J Neurosurg. 59:298–303. 1983.34. Yang W, Huang J. Chronic subdural hematoma: epidemiology and natural history. Neurosurg Clin N Am. 28:205–210. 2017.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular surgery for chronic subdural hematoma
- Usefulness of Middle Meningeal Embolization to Prevent Recurrent Spontaneous Chronic Subdural Hemorrhage
- Retrograde Middle Meningeal Artery Embolization through Mini Craniotomy for Subdural Hematoma Evacuation: A Technical Note
- Middle meningeal artery embolization for postoperative supratentorial chronic subdural hematoma occurring after posterior fossa neurosurgery
- Middle Meningeal Artery Embolization in Recurrent Chronic Subdural Hematoma Combined with Arachnoid Cyst
