Evaluation and Management of Bone Health in Patients with Thyroid Diseases: A Position Statement of the Korean Thyroid Association
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea
- KMID: 2541874
- DOI: http://doi.org/10.3803/EnM.2023.1701
Abstract
- Thyroid hormones play an important physiological role in maintaining adult bone structure and strength. Consequently, thyroid dysfunction is related to skeletal outcomes. Overt hyperthyroidism is an established cause of high bone turnover with accelerated bone loss, leading to osteoporosis and increased fracture risk. Hyperthyroidism induced by thyroid-stimulating hormone-suppressive therapy in patients with differentiated thyroid cancer is a cause of secondary osteoporosis. In contrast, there is a lack of evidence on the negative impact of hypothyroidism on bone health. Considering the clinical updates on the importance of bone health in thyroid dysfunction, the Task Force from the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association recently developed a position statement on the evaluation and management of bone health of patients with thyroid diseases, particularly focused on endogenous hyperthyroidism and thyroid-stimulating hormone-suppressive therapy-associated hyperthyroidism in patients with differentiated thyroid cancer. Herein, we review the Korean Thyroid Association’s position statement on the evaluation and management of bone health associated with thyroid diseases.
Figure
-
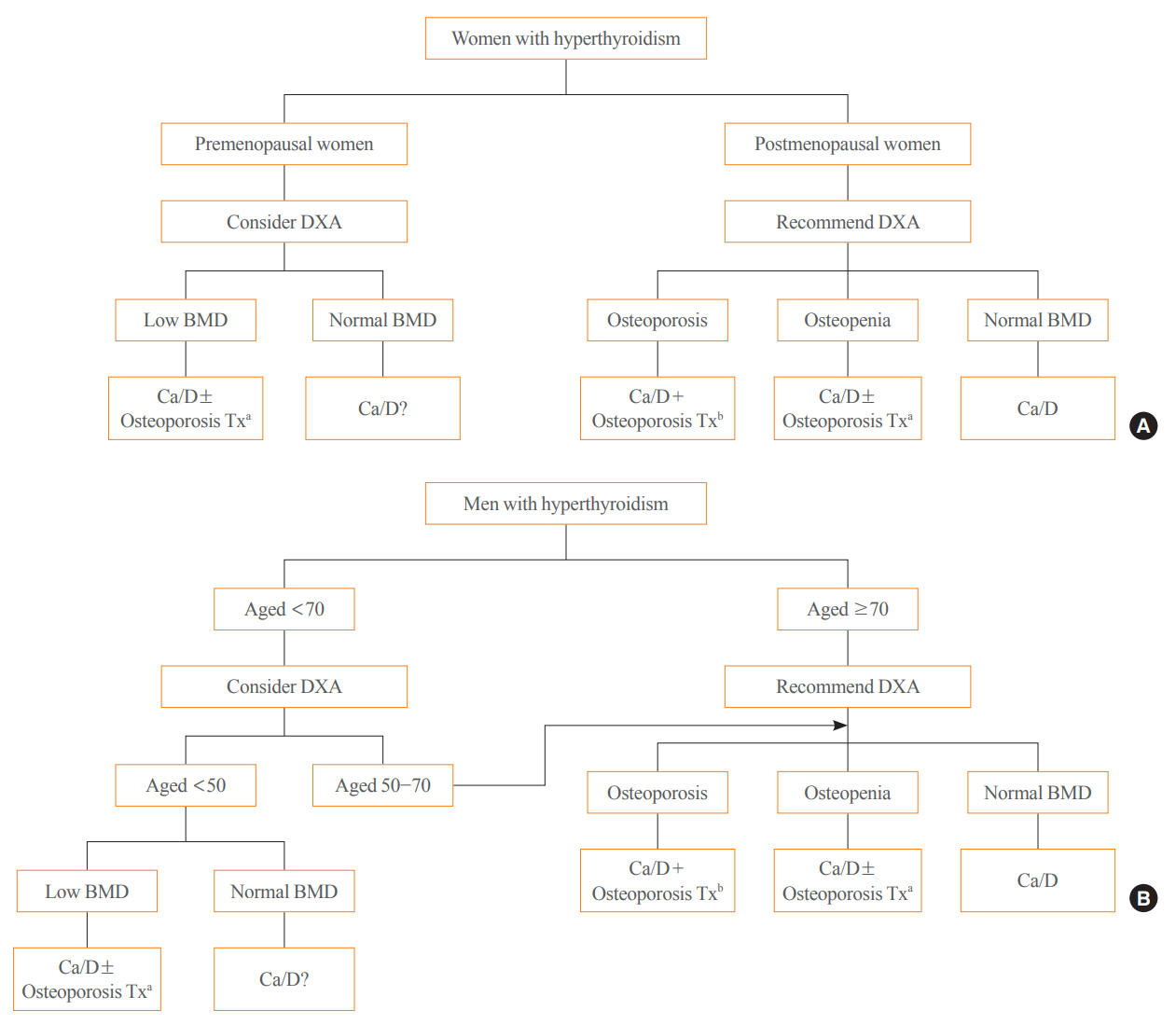
Fig. 1. Evaluation and management of bone health in (A) women and (B) men with hyperthyroidism. Anti-osteoporosis treatment includes therapy with anti-resorptive agents (e.g., bisphosphonates) and anabolic agents. Certain types of bisphosphonates (e.g., ibandronate) are not approved for men. DXA, dual-energy X-ray absorptiometry; BMD, bone mineral density; Ca/D, calcium and vitamin D; Tx, therapy. aCa/D±Osteoporosis Tx: Treatment for osteoporosis can be considered in combination with calcium and vitamin D replacement; bCa/D+Osteoporosis Tx: Treatment for osteoporosis is needed in combination with calcium and vitamin D replacement.
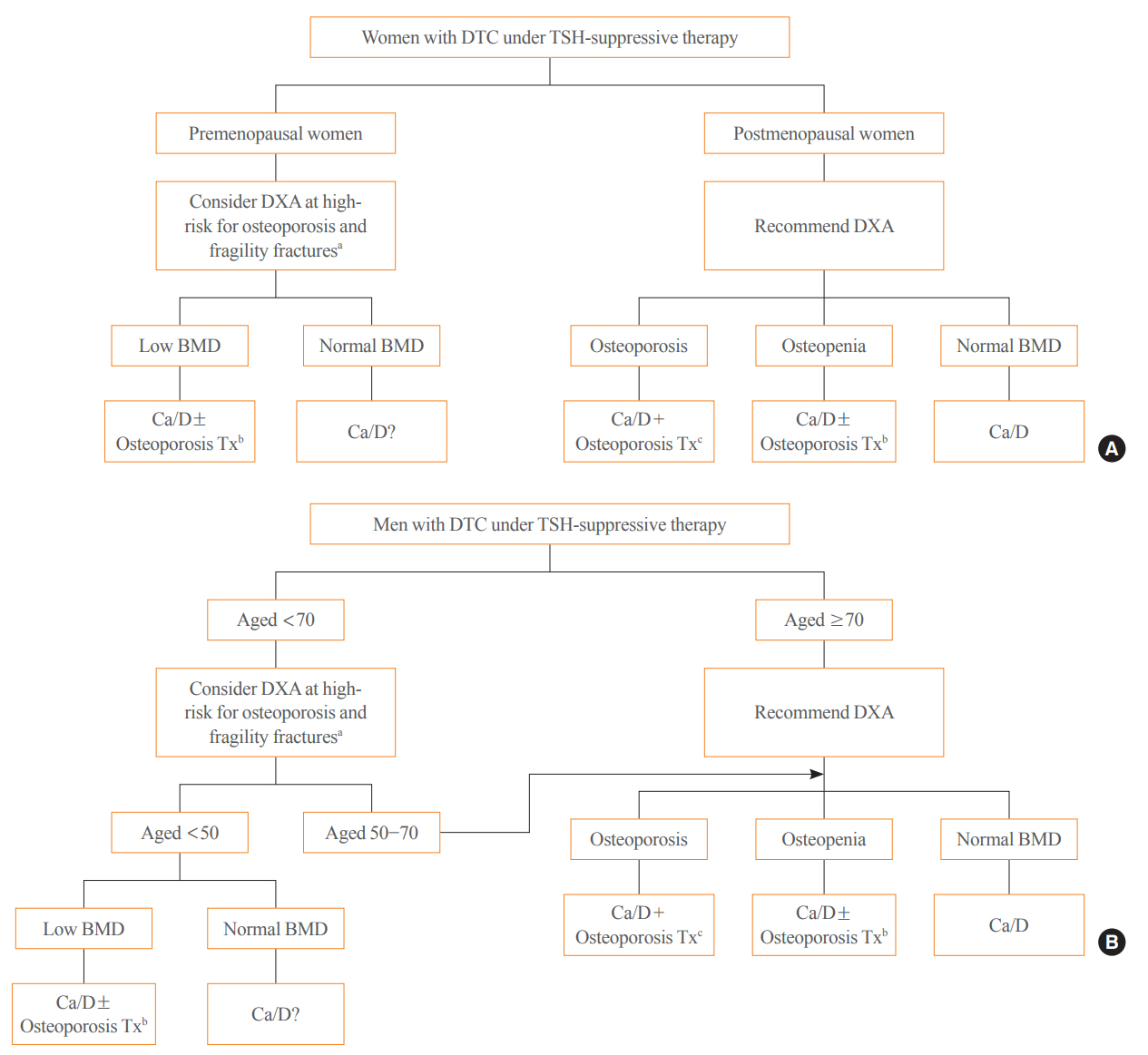
Fig. 2. Evaluation and management of bone health in (A) women and (B) men with differentiated thyroid cancer (DTC) receiving thyroidstimulating hormone (TSH)-suppressive therapy. Anti-osteoporosis treatment includes therapy with anti-resorptive agents (e.g., bisphosphonates) and anabolic agents. Certain types of bisphosphonates (e.g., ibandronate) are not approved for men. DXA, dual-energy X-ray absorptiometry; BMD, bone mineral density; Ca/D, calcium and vitamin D; Tx, therapy. aThe high-risk group for osteoporosis and fragility fractures had a previous history of fragility fractures, had amenorrhea for more than 1 year (for women), had other medical diseases, and took medications that cause osteoporosis; bCa/D±Osteoporosis Tx: Treatment for osteoporosis can be considered in combination with calcium and vitamin D replacement; cCa/D+Osteoporosis Tx: Treatment for osteoporosis is needed in combination with calcium and vitamin D replacement.
Reference
-
1. Wexler JA, Sharretts J. Thyroid and bone. Endocrinol Metab Clin North Am. 2007; 36:673–705.
Article2. Mundy GR, Shapiro JL, Bandelin JG, Canalis EM, Raisz LG. Direct stimulation of bone resorption by thyroid hormones. J Clin Invest. 1976; 58:529–34.
Article3. Kanatani M, Sugimoto T, Sowa H, Kobayashi T, Kanzawa M, Chihara K. Thyroid hormone stimulates osteoclast differentiation by a mechanism independent of RANKL-RANK interaction. J Cell Physiol. 2004; 201:17–25.
Article4. Vestergaard P, Mosekilde L. Fractures in patients with hyperthyroidism and hypothyroidism: a nationwide follow-up study in 16,249 patients. Thyroid. 2002; 12:411–9.
Article5. Uzzan B, Campos J, Cucherat M, Nony P, Boissel JP, Perret GY. Effects on bone mass of long term treatment with thyroid hormones: a meta-analysis. J Clin Endocrinol Metab. 1996; 81:4278–89.
Article6. Ross DS. Hyperthyroidism, thyroid hormone therapy, and bone. Thyroid. 1994; 4:319–26.
Article7. Heemstra KA, Hamdy NA, Romijn JA, Smit JW. The effects of thyrotropin-suppressive therapy on bone metabolism in patients with well-differentiated thyroid carcinoma. Thyroid. 2006; 16:583–91.
Article8. Cellini M, Rotondi M, Tanda ML, Piantanida E, Chiovato L, Beck-Peccoz P, et al. Skeletal health in patients with differentiated thyroid carcinoma. J Endocrinol Invest. 2021; 44:431–42.
Article9. Notsu M, Yamauchi M, Morita M, Nawata K, Sugimoto T. Papillary thyroid carcinoma is a risk factor for severe osteoporosis. J Bone Miner Metab. 2020; 38:264–70.
Article10. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016; 26:1–133.
Article11. Hong AR, Ahn HY, Kim BK, Ahn SH, Park SY, Kim MH, et al. Evaluation and management of bone health in patients with thyroid diseases: a position statement from the Korean Thyroid Association. Int J Thyroidol. 2022; 15:1–16.
Article12. Chin SO, Ku CR, Kim BJ, Kim SW, Park KH, Song KH, et al. Medical treatment with somatostatin analogues in acromegaly: position statement. Endocrinol Metab (Seoul). 2019; 34:53–62.
Article13. Ku EJ, Kim KJ, Kim JH, Kim MK, Ahn CH, Lee KA, et al. Diagnosis for pheochromocytoma and paraganglioma: a joint position statement of the Korean Pheochromocytoma and Paraganglioma Task Force. Endocrinol Metab (Seoul). 2021; 36:322–38.
Article14. Bassett JH, Williams GR. Role of thyroid hormones in skeletal development and bone maintenance. Endocr Rev. 2016; 37:135–87.
Article15. Abrahamsen B, Jorgensen HL, Laulund AS, Nybo M, Bauer DC, Brix TH, et al. The excess risk of major osteoporotic fractures in hypothyroidism is driven by cumulative hyperthyroid as opposed to hypothyroid time: an observational register-based time-resolved cohort analysis. J Bone Miner Res. 2015; 30:898–905.
Article16. Ko YJ, Kim JY, Lee J, Song HJ, Kim JY, Choi NK, et al. Levothyroxine dose and fracture risk according to the osteoporosis status in elderly women. J Prev Med Public Health. 2014; 47:36–46.
Article17. Mosekilde L, Eriksen EF, Charles P. Effects of thyroid hormones on bone and mineral metabolism. Endocrinol Metab Clin North Am. 1990; 19:35–63.
Article18. Mosekilde L, Melsen F, Bagger JP, Myhre-Jensen O, Schwartz Sorensen N. Bone changes in hyperthyroidism: interrelationships between bone morphometry, thyroid function and calcium-phosphorus metabolism. Acta Endocrinol (Copenh). 1977; 85:515–25.
Article19. Bours SP, van Geel TA, Geusens PP, Janssen MJ, Janzing HM, Hoffland GA, et al. Contributors to secondary osteoporosis and metabolic bone diseases in patients presenting with a clinical fracture. J Clin Endocrinol Metab. 2011; 96:1360–7.
Article20. Garnero P, Sornay-Rendu E, Claustrat B, Delmas PD. Biochemical markers of bone turnover, endogenous hormones and the risk of fractures in postmenopausal women: the OFELY study. J Bone Miner Res. 2000; 15:1526–36.
Article21. Bauer DC, Ettinger B, Nevitt MC, Stone KL; Study of Osteoporotic Fractures Research Group. Risk for fracture in women with low serum levels of thyroid-stimulating hormone. Ann Intern Med. 2001; 134:561–8.
Article22. Vestergaard P, Rejnmark L, Mosekilde L. Influence of hyper- and hypothyroidism, and the effects of treatment with antithyroid drugs and levothyroxine on fracture risk. Calcif Tissue Int. 2005; 77:139–44.
Article23. Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, et al. Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl J Med. 1995; 332:767–73.24. Wejda B, Hintze G, Katschinski B, Olbricht T, Benker G. Hip fractures and the thyroid: a case-control study. J Intern Med. 1995; 237:241–7.
Article25. Vestergaard P, Mosekilde L. Hyperthyroidism, bone mineral, and fracture risk: a meta-analysis. Thyroid. 2003; 13:585–93.
Article26. Dhanwal DK, Gupta N. Bone mineral density trends in Indian patients with Hyperthyroidism: effect of antithyroid therapy. J Assoc Physicians India. 2011; 59:561–567. 561-2, 567.27. Marshall D, Johnell O, Wedel H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ. 1996; 312:1254–9.28. Torgerson DJ, Campbell MK, Thomas RE, Reid DM. Prediction of perimenopausal fractures by bone mineral density and other risk factors. J Bone Miner Res. 1996; 11:293–7.29. Camacho PM, Petak SM, Binkley N, Diab DL, Eldeiry LS, Farooki A, et al. American Association of Clinical Endocrinologists/American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis: 2020 update. Endocr Pract. 2020; 26(Suppl 1):1–46.30. Shoback D, Rosen CJ, Black DM, Cheung AM, Murad MH, Eastell R. Pharmacological management of osteoporosis in postmenopausal women: an endocrine society guideline update. J Clin Endocrinol Metab. 2020; 105:dgaa048.31. The Korean Society for Bone and Mineral Research. Physician’s guideline for osteoporosis. Seoul: Korean Society for Bone and Mineral Research;2020.32. Udayakumar N, Chandrasekaran M, Rasheed MH, Suresh RV, Sivaprakash S. Evaluation of bone mineral density in thyrotoxicosis. Singapore Med J. 2006; 47:947–50.33. Ale AO, Ogbera AO, Ebili HO, Adeyemo OL, Afe TO. Prevalence, predictive factors, and characteristics of osteoporosis in hyperthyroid patients. Int J Endocrinol. 2018; 2018:3540256.
Article34. Kuzma M, Vanuga P, Binkley N, Sagova I, Pavai D, Blazicek P, et al. High serum fractalkine is associated with lower trabecular bone score in premenopausal women with Graves’ disease. Horm Metab Res. 2018; 50:609–14.
Article35. Boonya-Ussadorn T, Punkaew B, Sriassawaamorn N. A comparative study of bone mineral density between premenopausal women with hyperthyroidism and healthy premenopausal women. J Med Assoc Thai. 2010; 93 Suppl 6:S1–5.36. Garnero P, Vassy V, Bertholin A, Riou JP, Delmas PD. Markers of bone turnover in hyperthyroidism and the effects of treatment. J Clin Endocrinol Metab. 1994; 78:955–9.
Article37. Harvey RD, McHardy KC, Reid IW, Paterson F, Bewsher PD, Duncan A, et al. Measurement of bone collagen degradation in hyperthyroidism and during thyroxine replacement therapy using pyridinium cross-links as specific urinary markers. J Clin Endocrinol Metab. 1991; 72:1189–94.
Article38. Kisakol G, Kaya A, Gonen S, Tunc R. Bone and calcium metabolism in subclinical autoimmune hyperthyroidism and hypothyroidism. Endocr J. 2003; 50:657–61.
Article39. Sabuncu T, Aksoy N, Arikan E, Ugur B, Tasan E, Hatemi H. Early changes in parameters of bone and mineral metabolism during therapy for hyper- and hypothyroidism. Endocr Res. 2001; 27:203–13.
Article40. Olkawa M, Kushida K, Takahashi M, Ohishi T, Hoshino H, Suzuki M, et al. Bone turnover and cortical bone mineral density in the distal radius in patients with hyperthyroidism being treated with antithyroid drugs for various periods of time. Clin Endocrinol (Oxf). 1999; 50:171–6.
Article41. Karunakaran P, Maharajan C, Mohamed KN, Rachamadugu SV. Rapid restoration of bone mass after surgical management of hyperthyroidism: a prospective case control study in Southern India. Surgery. 2016; 159:771–6.
Article42. Kumeda Y, Inaba M, Tahara H, Kurioka Y, Ishikawa T, Morii H, et al. Persistent increase in bone turnover in Graves’ patients with subclinical hyperthyroidism. J Clin Endocrinol Metab. 2000; 85:4157–61.
Article43. Zhong N, Xu B, Cui R, Xu M, Su J, Zhang Z, et al. Positive correlation between serum osteocalcin and testosterone in male hyperthyroidism patients with high bone turnover. Exp Clin Endocrinol Diabetes. 2016; 124:452–6.
Article44. Ock SY, Chung YS, Choi YJ. Changes in bone mineral density and trabecular bone score in Graves’ disease patients after anti-thyroid therapy. Osteoporos Sarcopenia. 2016; 2:175–9.
Article45. Nicolaisen P, Obling ML, Winther KH, Hansen S, Hermann AP, Hegedus L, et al. Consequences of hyperthyroidism and its treatment for bone microarchitecture assessed by high-resolution peripheral quantitative computed tomography. Thyroid. 2021; 31:208–16.
Article46. Grant AM, Avenell A, Campbell MK, McDonald AM, MacLennan GS, McPherson GC, et al. Oral vitamin D3 and calcium for secondary prevention of low-trauma fractures in elderly people (Randomised Evaluation of Calcium Or vitamin D, RECORD): a randomised placebo-controlled trial. Lancet. 2005; 365:1621–8.
Article47. Tang BM, Eslick GD, Nowson C, Smith C, Bensoussan A. Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: a meta-analysis. Lance. 2007; 370:657–66.
Article48. Weaver CM, Fleet JC. Vitamin D requirements: current and future. Am J Clin Nutr. 2004; 80(6 Suppl):1735S–9S.
Article49. Avenell A, Gillespie WJ, Gillespie LD, O’Connell D. Vitamin D and vitamin D analogues for preventing fractures associated with involutional and post-menopausal osteoporosis. Cochrane Database Syst Rev. 2009; 2:CD000227.
Article50. Kim KM, Choi SH, Lim S, Moon JH, Kim JH, Kim SW, et al. Interactions between dietary calcium intake and bone mineral density or bone eometry in a low calcium intake population (KNHANES IV 2008-2010). J Clin Endocrinol Metab. 2014; 99:2409–17.51. Park JH, Hong IY, Chung JW, Choi HS. Vitamin D status in South Korean population: seven-year trend from the KNHANES. Medicine (Baltimore). 2018; 97:e11032.52. Lupoli G, Nuzzo V, Di Carlo C, Affinito P, Vollery M, Vitale G, et al. Effects of alendronate on bone loss in pre- and postmenopausal hyperthyroid women treated with methimazole. Gynecol Endocrinol. 1996; 10:343–8.
Article53. Lupoli GA, Fittipaldi MR, Fonderico F, Panico A, Colarusso S, Di Micco L, et al. Methimazole versus methimazole and diphosphonates in hyperthyroid and osteoporotic patients. Minerva Endocrinol. 2005; 30:89–94.54. Majima T, Komatsu Y, Doi K, Takagi C, Shigemoto M, Fukao A, et al. Clinical significance of risedronate for osteoporosis in theinitial treatment of male patients with Graves’ disease. J Bone Miner Metab. 2006; 24:105–13.
Article55. Kanis JA, Hans D, Cooper C, Baim S, Bilezikian JP, Binkley N, et al. Interpretation and use of FRAX in clinical practice. Osteoporos Int. 2011; 22:2395–411.
Article56. Cooper DS, Biondi B. Subclinical thyroid disease. Lancet. 2012; 379:1142–54.
Article57. Amato G, Mazziotti G, Sorvillo F, Piscopo M, Lalli E, Biondi B, et al. High serum osteoprotegerin levels in patients with hyperthyroidism: effect of medical treatment. Bone. 2004; 35:785–91.
Article58. Gurlek A, Gedik O. Effect of endogenous subclinical hyperthyroidism on bone metabolism and bone mineral density in premenopausal women. Thyroid. 1999; 9:539–43.
Article59. Tauchmanova L, Nuzzo V, Del Puente A, Fonderico F, Esposito-Del Puente A, Padulla S, et al. Reduced bone mass detected by bone quantitative ultrasonometry and DEXA in pre- and postmenopausal women with endogenous subclinical hyperthyroidism. Maturitas. 2004; 48:299–306.
Article60. Lee WY, Oh KW, Rhee EJ, Jung CH, Kim SW, Yun EJ, et al. Relationship between subclinical thyroid dysfunction and femoral neck bone mineral density in women. Arch Med Res. 2006; 37:511–6.
Article61. Wartofsky L. Subclinical hyperthyroidism and fracture risk in women. J Clin Endocrinol Metab. 2014; 99:2654–6.
Article62. Foldes J, Tarjan G, Szathmari M, Varga F, Krasznai I, Horvath C. Bone mineral density in patients with endogenous subclinical hyperthyroidism: is this thyroid status a risk factor for osteoporosis? Clin Endocrinol (Oxf). 1993; 39:521–7.
Article63. Faber J, Jensen IW, Petersen L, Nygaard B, Hegedus L, Siersbaek-Nielsen K. Normalization of serum thyrotrophin by means of radioiodine treatment in subclinical hyperthyroidism: effect on bone loss in postmenopausal women. Clin Endocrinol (Oxf). 1998; 48:285–90.
Article64. Yan Z, Huang H, Li J, Wang J. Relationship between subclinical thyroid dysfunction and the risk of fracture: a metaanalysis of prospective cohort studies. Osteoporos Int. 2016; 27:115–25.
Article65. Saler T, Ahbab S, Saglam ZA, Keskek SO, Kurnaz S. Endogenous subclinical hyperthyroidism may not lead to bone loss in premenopausal women. Hippokratia. 2014; 18:240–4.66. Nicholls JJ, Brassill MJ, Williams GR, Bassett JH. The skeletal consequences of thyrotoxicosis. J Endocrinol. 2012; 213:209–21.
Article67. Lee JS, Buzkova P, Fink HA, Vu J, Carbone L, Chen Z, et al. Subclinical thyroid dysfunction and incident hip fracture in older adults. Arch Intern Med. 2010; 170:1876–83.
Article68. Blum MR, Bauer DC, Collet TH, Fink HA, Cappola AR, da Costa BR, et al. Subclinical thyroid dysfunction and fracture risk: a meta-analysis. JAMA. 2015; 313:2055–65.69. Wirth CD, Blum MR, da Costa BR, Baumgartner C, Collet TH, Medici M, et al. Subclinical thyroid dysfunction and the risk for fractures: a systematic review and meta-analysis. Ann Intern Med. 2014; 161:189–99.
Article70. Faber J, Galloe AM. Changes in bone mass during prolonged subclinical hyperthyroidism due to L-thyroxine treatment: a meta-analysis. Eur J Endocrinol. 1994; 130:350–6.
Article71. Papaleontiou M, Hawley ST, Haymart MR. Effect of thyrotropin suppression therapy on bone in thyroid cancer patients. Oncologist. 2016; 21:165–71.
Article72. Yoon BH, Lee Y, Oh HJ, Kim SH, Lee YK. Influence of thyroid-stimulating hormone suppression therapy on bone mineral density in patients with differentiated thyroid cancer: a meta-analysis. J Bone Metab. 2019; 26:51–60.
Article73. Wang MY, Han ZQ, Gong XW, Li Q, Ma J. TSH-suppressive therapy can reduce bone mineral density in patients with differentiated thyroid carcinoma: a meta-analysis. Eur Rev Med Pharmacol Sci. 2020; 24:922–9.74. Ku EJ, Yoo WS, Lee EK, Ahn HY, Woo SH, Hong JH, et al. Effect of TSH suppression therapy on bone mineral density in differentiated thyroid cancer: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2021; 106:3655–67.
Article75. Kwak D, Ha J, Won Y, Kwon Y, Park S. Effects of thyroid-stimulating hormone suppression after thyroidectomy for thyroid cancer on bone mineral density in postmenopausal women: a systematic review and meta-analysis. BMJ Open. 2021; 11:e043007.
Article76. Mazziotti G, Formenti AM, Frara S, Olivetti R, Banfi G, Memo M, et al. High prevalence of radiological vertebral fractures in women on thyroid-stimulating hormone-suppressive therapy for thyroid carcinoma. J Clin Endocrinol Metab. 2018; 103:956–64.
Article77. Fujiyama K, Kiriyama T, Ito M, Kimura H, Ashizawa K, Tsuruta M, et al. Suppressive doses of thyroxine do not accelerate age-related bone loss in late postmenopausal women. Thyroid. 1995; 5:13–7.
Article78. Heijckmann AC, Huijberts MS, Geusens P, de Vries J, Menheere PP, Wolffenbuttel BH. Hip bone mineral density, bone turnover and risk of fracture in patients on long-term suppressive L-thyroxine therapy for differentiated thyroid carcinoma. Eur J Endocrinol. 2005; 153:23–9.
Article79. Reverter JL, Colome E, Holgado S, Aguilera E, Soldevila B, Mateo L, et al. Bone mineral density and bone fracture in male patients receiving long-term suppressive levothyroxine treatment for differentiated thyroid carcinoma. Endocrine. 2010; 37:467–72.
Article80. Vera L, Gay S, Campomenosi C, Paolino S, Pera G, Monti E, et al. Ten-year estimated risk of bone fracture in women with differentiated thyroid cancer under TSH-suppressive levothyroxine therapy. Endokrynol Pol. 2016; 67:350–8.
Article81. Lin SY, Lin CL, Chen HT, Kao CH. Risk of osteoporosis in thyroid cancer patients using levothyroxine: a population-based study. Curr Med Res Opin. 2018; 34:805–12.
Article82. Shin DW, Suh B, Lim H, Yun JM, Song SO, Park Y. J-shaped association between postoperative levothyroxine dosage and fracture risk in thyroid cancer patients: a retrospective cohort study. J Bone Miner Res. 2018; 33:1037–43.
Article83. Bin-Hong D, Fu-Man D, Yu L, Xu-Ping W, Bing-Feng B. Effects of levothyroxine therapy on bone mineral density and bone turnover markers in premenopausal women with thyroid cancer after thyroidectomy. Endokrynol Pol. 2020; 71:15–20.
Article84. Lee MY, Park JH, Bae KS, Jee YG, Ko AN, Han YJ, et al. Bone mineral density and bone turnover markers in patients on long-term suppressive levothyroxine therapy for differentiated thyroid cancer. Ann Surg Treat Res. 2014; 86:55–60.
Article85. Moon JH, Kim KM, Oh TJ, Choi SH, Lim S, Park YJ, et al. The effect of TSH suppression on vertebral trabecular bone scores in patients with differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2017; 102:78–85.86. De Mingo Dominguez ML, Guadalix Iglesias S, Martin-Arriscado Arroba C, Lopez Alvarez B, Martinez Diaz-Guerra G, Martinez-Pueyo JI, et al. Low trabecular bone score in postmenopausal women with differentiated thyroid carcinoma after long-term TSH suppressive therapy. Endocrine. 2018; 62:166–73.
Article87. Hawkins Carranza F, Guadalix Iglesias S, Luisa De Mingo Dominguez M, Martin-Arriscado Arroba C, Lopez Alvarez B, Allo Miguel G, et al. Trabecular bone deterioration in differentiated thyroid cancer: impact of long-term TSH suppressive therapy. Cancer Med. 2020; 9:5746–55.
Article88. Moon JH, Jung KY, Kim KM, Choi SH, Lim S, Park YJ, et al. The effect of thyroid stimulating hormone suppressive therapy on bone geometry in the hip area of patients with differentiated thyroid carcinoma. Bone. 2016; 83:104–10.
Article89. Tournis S, Antoniou JD, Liakou CG, Christodoulou J, Papakitsou E, Galanos A, et al. Volumetric bone mineral density and bone geometry assessed by peripheral quantitative computed tomography in women with differentiated thyroid cancer under TSH suppression. Clin Endocrinol (Oxf). 2015; 82:197–204.
Article90. Kim K, Kim IJ, Pak K, Kim SJ, Shin S, Kim BH, et al. Evaluation of bone mineral density using DXA and cQCT in postmenopausal patients under thyrotropin suppressive therapy. J Clin Endocrinol Metab. 2018; 103:4232–40.
Article91. Panico A, Lupoli GA, Fonderico F, Marciello F, Martinelli A, Assante R, et al. Osteoporosis and thyrotropin-suppressive therapy: reduced effectiveness of alendronate. Thyroid. 2009; 19:437–42.
Article92. Panebianco P, Rosso D, Destro G, Scarpinato RA, Tropea S, Rizzo A, et al. Use of disphosphonates in the treatment of osteoporosis in thyroidectomized patients on levothyroxine replacement therapy. Arch Gerontol Geriatr. 1997; 25:219–25.93. Asari R, Passler C, Kaczirek K, Scheuba C, Niederle B. Hypoparathyroidism after total thyroidectomy: a prospective study. Arch Surg. 2008; 143:132–7.94. Pattou F, Combemale F, Fabre S, Carnaille B, Decoulx M, Wemeau JL, et al. Hypocalcemia following thyroid surgery: incidence and prediction of outcome. World J Surg. 1998; 22:718–24.
Article95. Röher HD, Goretzki PE, Hellmann P, Witte J. Complications in thyroid surgery. Incidence and therapy. Chirurg. 1999; 70:999–1010.96. Thomusch O, Machens A, Sekulla C, Ukkat J, Brauckhoff M, Dralle H. The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: a multivariate analysis of 5846 consecutive patients. Surgery. 2003; 133:180–5.97. Thomusch O, Machens A, Sekulla C, Ukkat J, Lippert H, Gastinger I, et al. Multivariate analysis of risk factors for postoperative complications in benign goiter surgery: prospective multicenter study in Germany. World J Surg. 2000; 24:1335–41.98. Testini M, Gurrado A, Lissidini G, Nacchiero M. Hypoparathyroidism after total thyroidectomy. Minerva Chir. 2007; 62:409–15.99. Kakava K, Tournis S, Papadakis G, Karelas I, Stampouloglou P, Kassi E, et al. Postsurgical hypoparathyroidism: a systematic review. In Vivo. 2016; 30:171–9.100. Bilezikian JP, Marcus R, Levine MA, Marcocci C, Silver-berg SJ, Potts JT. The parathyroids: basic and clinical concepts. 3rd ed. London: Elsevier Inc;2015. Chapter 8, Cellular actions of PTH: osteoblasts, osteoclasts, and osteocytes. p. 127–37.101. Rubin MR, Dempster DW, Zhou H, Shane E, Nickolas T, Sliney J Jr, et al. Dynamic and structural properties of the skeleton in hypoparathyroidism. J Bone Miner Res. 2008; 23:2018–24.102. Clarke BL. Bone disease in hypoparathyroidism. Arq Bras Endocrinol Metabol. 2014; 58:545–52.
Article103. Chan FK, Tiu SC, Choi KL, Choi CH, Kong AP, Shek CC. Increased bone mineral density in patients with chronic hypoparathyroidism. J Clin Endocrinol Metab. 2003; 88:3155–9.
Article104. Amrein K, Dimai HP, Dobnig H, Fahrleitner-Pammer A. Low bone turnover and increase of bone mineral density in a premenopausal woman with postoperative hypoparathyroidism and thyroxine suppressive therapy. Osteoporos Int. 2011; 22:2903–5.
Article105. Takamura Y, Miyauchi A, Yabuta T, Kihara M, Ito Y, Miya A. Attenuation of postmenopausal bone loss in patients with transient hypoparathyroidism after total thyroidectomy. World J Surg. 2013; 37:2860–5.
Article106. Bollerslev J, Rejnmark L, Marcocci C, Shoback DM, Sitges-Serra A, van Biesen W, et al. European Society of Endocrinology clinical guideline: treatment of chronic hypoparathyroidism in adults. Eur J Endocrinol. 2015; 173:G1–20.
Article107. Orloff LA, Wiseman SM, Bernet VJ, Fahey TJ 3rd, Shaha AR, Shindo ML, et al. American Thyroid Association statement on postoperative hypoparathyroidism: diagnosis, prevention, and management in adults. Thyroid. 2018; 28:830–41.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation and Management of Bone Health in Patients with Thyroid Diseases: a Position Statement from the Korean Thyroid Association
- The Management of Thyroid Disease in COVID-19 Pandemic
- Consensus Position Statement of Korean Endocrine Society and Korean Thyroid Association
- Thyroid disease in pregnancy
- Treatment of Thyroid Nodule
