Acute allograft dysfunction mimicking thrombotic microangiopathy in kidney transplant recipient with renal infarction: case report and review of literatures
- Affiliations
-
- 1Division of Nephrology, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- 2Department of Medicine and Geriatrics, Kwong Wah Hospital, Hong Kong, China
- 3Transplant Research Center, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 4Division of Nephrology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 5Division of Vascular and Transplant Surgery, Department of Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2510266
- DOI: http://doi.org/10.4285/kjt.20.0034
Abstract
- Acute allograft dysfunction is rarely observed in kidney transplantation (KT). We report an unusual case of acute allograft dysfunction mimicking thrombotic microangiopa- thy (TMA) in recipient with renal infarction. A 65-year-old man underwent KT from his 39-year-old son. Pre-transplant donor evaluation was normal except for the branches of the upper and lower pole renal arteries originating from the aorta in renal computed topographic angiography, respectively. The immediate post-transplant clinical course was uneventful, but serum creatinine (SCr) increased from 2.2 to 4.5 mg/dL, anemia and throm-bocytopenia were shown, and serum lactate dehydrogenase increased to 919 U/L on the third day after transplantation. We suspected TMA, because of no evidence of acute bleeding. The laboratory parameters associated with TMA were within normal ranges. Renal magnetic resonance angiography revealed a focal wedge-shaped perfusion defect in the upper pole of the graft and renal Doppler ultrasonography showed decreased per- fusion of the lower pole of the graft. Graft function improved with conservative therapy. The patient was discharged with SCr of 1.21 mg/dL. Graft function has been stable after discharge. Acute allograft infarction should be considered in the differential diagnosis of acute allograft dysfunction mimicking TMA in recipients with grafts supplied by multiple renal arteries.
Figure
-
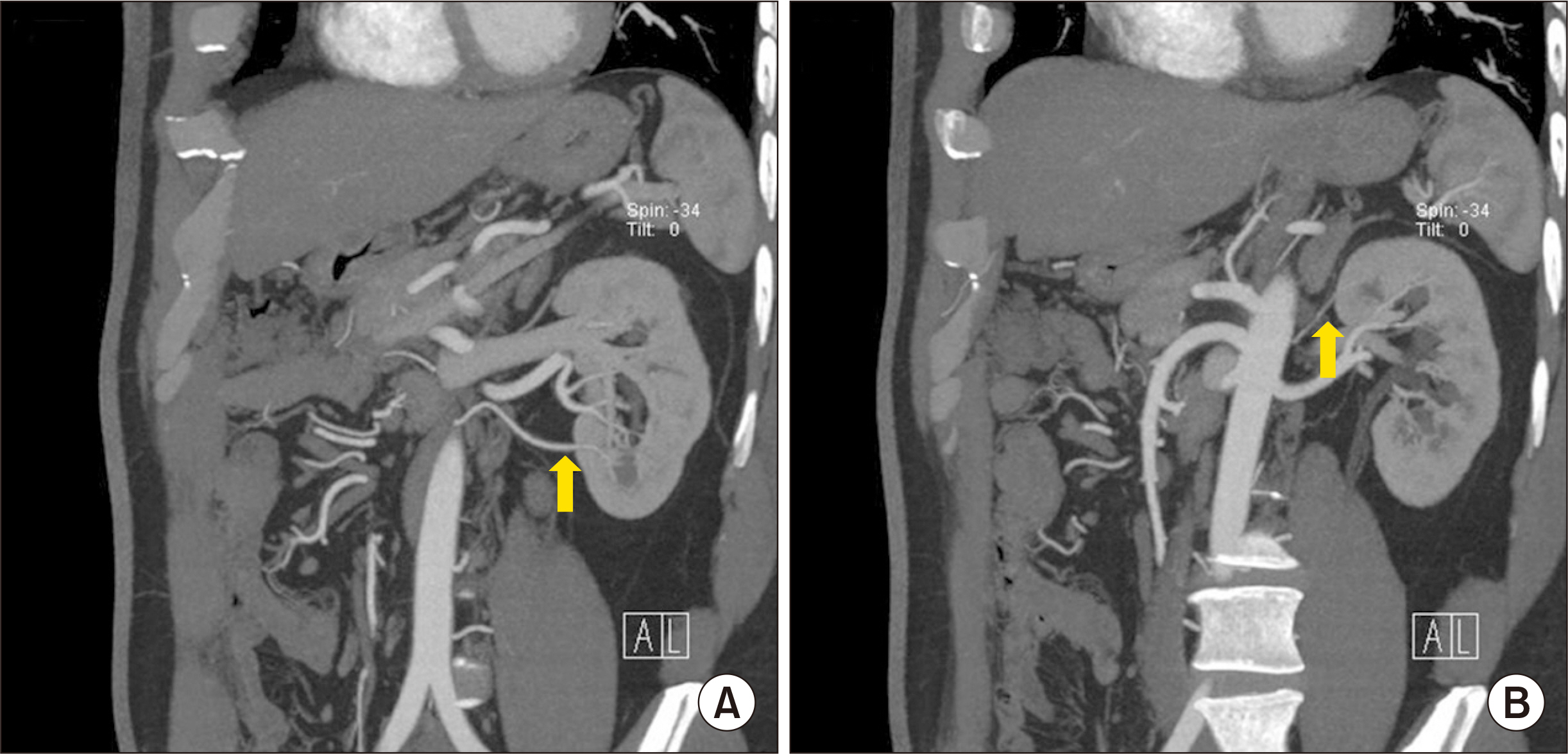
Fig. 1 Renal computed tomography angiogram of the donor. A small lower polar branch arises from the aorta (arrow), supplying the lower pole (A) and a tiny upper polar branch arises from the aorta (arrow), supplying the upper pole of the left kidney (B).
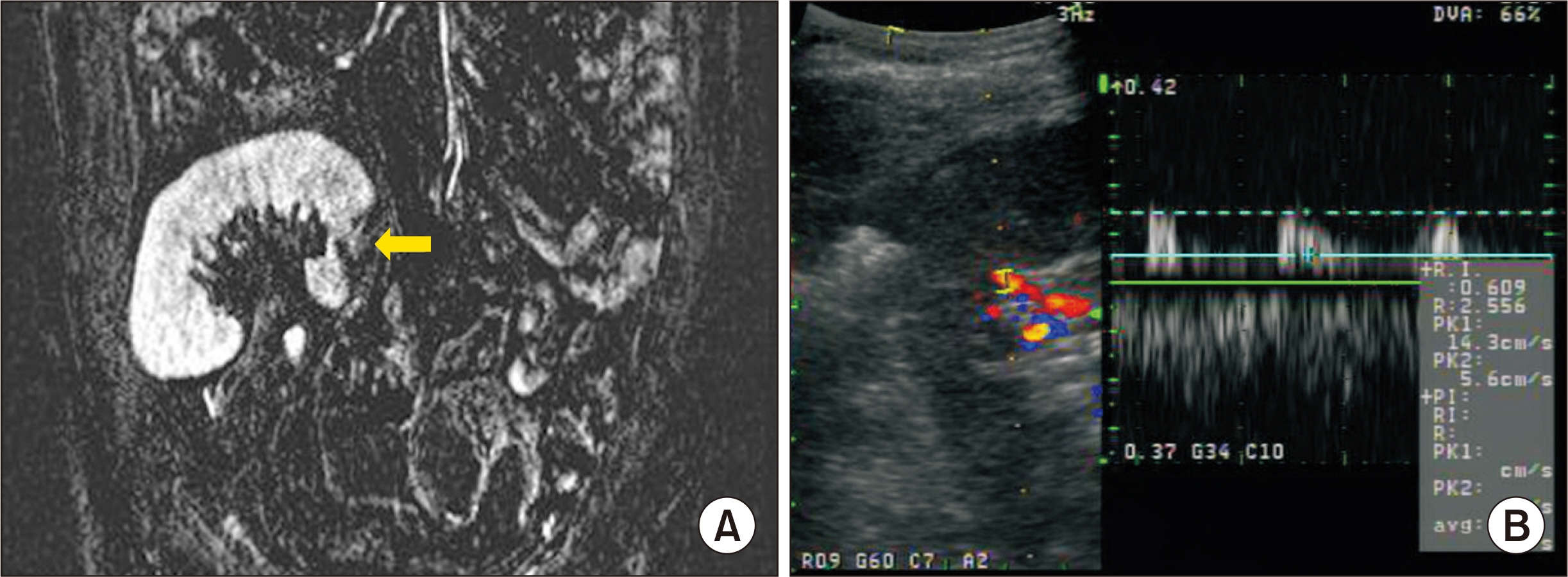
Fig. 2 Radiologic findings of the recipient. Focal wedge shaped perfusion defect in the upper pole of the transplanted kidney on flair images (arrow), coronal view of renal magnetic resonance angiography (A) and slightly decreased vascularity and perfusion in inferior pole of graft kidney on kidney Doppler ultrasonography (B). Peak systolic velocity of lower inter-lobar artery reduced to 14.3 cm/sec.
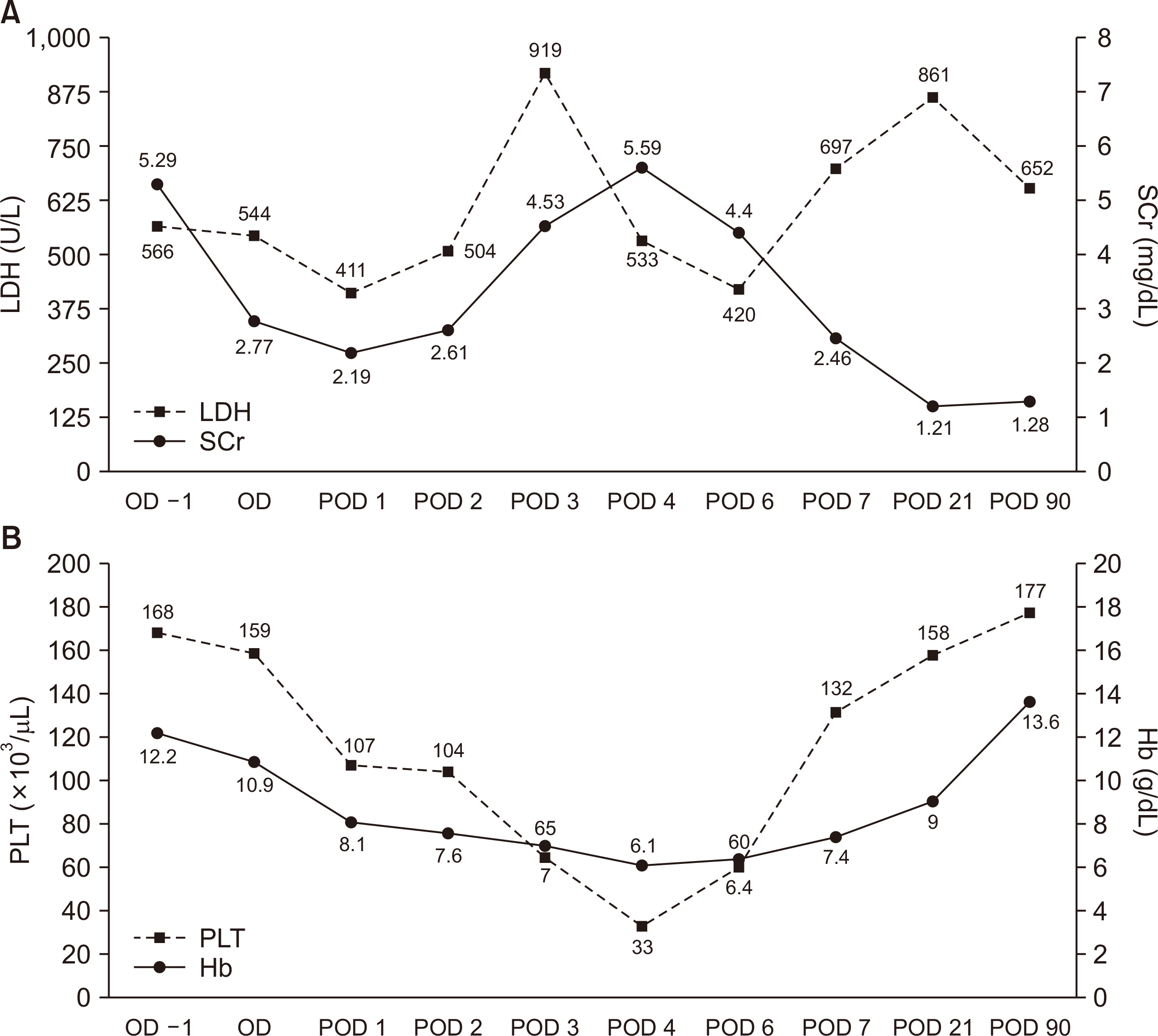
Fig. 3 Change of laboratory findings after kidney transplantation. (A) On the 1st day after transplantation, serum creatinine (SCr) decreased to 2.19 mg/dL. However, on the 2nd day after transplantation, SCr began to increase and reached to 5.59 mg/dL on the 4th day after transplantation. At the same time, serum lactate dehydrogenase (LDH) also increased to 919 U/L. SCr recovered to 1.21 mg/dL on the day of discharge. (B) Serum hemoglobin (Hb) decreased from 10.9 g/dL to 7 g/dL for 3 days after transplantation. At the same time, serum platelet (PLT) count decreased from 159×103/µL to 65×103/µL. Serum Hb and PLT count recovered to normal with allograft renal function. OD, operative day; POD, postoperative day.
Reference
-
1. Sharma SG, Post JB, Herlitz LC, Markowitz G. 2013; Renal cortical infarction following treatment with sumatriptan in a kidney allograft recipient. Am J Kidney Dis. 61:326–9. DOI: 10.1053/j.ajkd.2012.07.032. PMID: 23206532.
Article2. Domanovits H, Paulis M, Nikfardjam M, Meron G, Kürkciyan I, Bankier AA, et al. 1999; Acute renal infarction. Clinical characteristics of 17 patients. Medicine (Baltimore). 78:386–94. DOI: 10.1097/00005792-199911000-00004. PMID: 10575421.3. Huang CC, Lo HC, Huang HH, Kao WF, Yen DH, Wang LM, et al. 2007; ED presentations of acute renal infarction. Am J Emerg Med. 25:164–9. DOI: 10.1016/j.ajem.2006.06.010. PMID: 17276805.
Article4. Chu PL, Wei YF, Huang JW, Chen SI, Chu TS, Wu KD. 2006; Clinical characteristics of patients with segmental renal infarction. Nephrology (Carlton). 11:336–40. DOI: 10.1111/j.1440-1797.2006.00586.x. PMID: 16889574.
Article5. Nadasdy T. 2014; Thrombotic microangiopathy in renal allografts: the diagnostic challenge. Curr Opin Organ Transplant. 19:283–92. DOI: 10.1097/MOT.0000000000000074. PMID: 24811438.6. Goldberg RJ, Weng FL, Kandula P. 2016; Acute and chronic allograft dysfunction in kidney transplant recipients. Med Clin North Am. 100:487–503. DOI: 10.1016/j.mcna.2016.01.002. PMID: 27095641.
Article7. Reynolds JC, Agodoa LY, Yuan CM, Abbott KC. 2003; Thrombotic microangiopathy after renal transplantation in the United States. Am J Kidney Dis. 42:1058–68. DOI: 10.1016/j.ajkd.2003.07.008. PMID: 14582050.8. Harmon WE, Stablein D, Alexander SR, Tejani A. 1991; Graft thrombosis in pediatric renal transplant recipients. A report of the North American Pediatric Renal Transplant Cooperative Study. Transplantation. 51:406–12. DOI: 10.1097/00007890-199102000-00026. PMID: 1994535.
Article9. Lee HM, Mendez-Picon G, Pierce JC, Hume DM. 1977; Renal artery occlusion in transplant recipients. Am Surg. 43:186–92. PMID: 320927.10. Venkateswara K, Smith EJ, Alexander JW, Fidler JP, Pemmaraju SR, Pollack VE. 1976; Thromboembolic disease in renal allograft recipients. What is its clinical significance? Arch Surg. 111:1086–92. DOI: 10.1001/archsurg.1976.01360280044007. PMID: 788676.11. Rijksen JF, Koolen MI, Walaszewski JE, Terpstra JL, Vink M. 1982; Vascular complications in 400 consecutive renal allotransplants. J Cardiovasc Surg (Torino). 23:91–8. PMID: 7045134.12. Kanchanabat B, Siddins M, Coates T, Tie M, Russell CH, Mathew T, et al. 2002; Segmental infarction with graft dysfunction: an emerging syndrome in renal transplantation? Nephrol Dial Transplant. 17:123–8. DOI: 10.1093/ndt/17.1.123. PMID: 11773475.
Article13. Oh YK, Yang CW, Kim YL, Kang SW, Park CW, Kim YS, et al. 2016; Clinical characteristics and outcomes of renal infarction. Am J Kidney Dis. 67:243–50. DOI: 10.1053/j.ajkd.2015.09.019. PMID: 26545635.
Article14. Singh A, Stablein D, Tejani A. 1997; Risk factors for vascular thrombosis in pediatric renal transplantation: a special report of the North American Pediatric Renal Transplant Cooperative Study. Transplantation. 63:1263–7. DOI: 10.1097/00007890-199705150-00012. PMID: 9158019.15. Pollak R, Prusak BF, Mozes MF. 1986; Anatomic abnormalities of cadaver kidneys procured for purposes of transplantation. Am Surg. 52:233–5. PMID: 3518559.16. Ozkan U, Oğuzkurt L, Tercan F, Kizilkiliç O, Koç Z, Koca N. 2006; Renal artery origins and variations: angiographic evaluation of 855 consecutive patients. Diagn Interv Radiol. 12:183–6. PMID: 17160802.17. Aydin C, Berber I, Altaca G, Yigit B, Titiz I. 2004; The outcome of kidney transplants with multiple renal arteries. BMC Surg. 4:4. DOI: 10.1186/1471-2482-4-4. PMID: 15018624. PMCID: PMC362880.
Article18. Gawish AE, Donia F, Samhan M, Halim MA, Al-Mousawi M. 2007; Outcome of renal allografts with multiple arteries. Transplant Proc. 39:1116–7. DOI: 10.1016/j.transproceed.2007.03.067. PMID: 17524906.
Article19. Ghazanfar A, Tavakoli A, Zaki MR, Pararajasingam R, Campbell T, Parrott NR, et al. 2010; The outcomes of living donor renal transplants with multiple renal arteries: a large cohort study with a mean follow-up period of 10 years. Transplant Proc. 42:1654–8. DOI: 10.1016/j.transproceed.2009.12.067. PMID: 20620494.
Article20. Hwang JK, Kim SD, Park SC, Choi BS, Kim JI, Yang CW, et al. 2010; The long-term outcomes of transplantation of kidneys with multiple renal arteries. Transplant Proc. 42:4053–7. DOI: 10.1016/j.transproceed.2010.09.075. PMID: 21168625.
Article21. Erenler KA, Duran L, Erenler BH, Baş Y, Yilmaz ZC. 2015; Diagnosis and management of renal infarction in the emergency department: a review. J Nephrol Urol. 3:13–7. DOI: 10.12970/2310-984X.2015.03.01.3.22. Voss DM, Bailey RR, Gardner J, Chisholm RJ. 1994; Diagnosis of cortical infarction in a renal transplant using ultrasonography. Nephron. 68:378–9. DOI: 10.1159/000188404. PMID: 7838264.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Antiphospholipid Syndrome Presenting as Recurrent Pancreatitis and Renal Thrombotic Microangiopathy
- A Case of Late Renal Transplant Segmental Infarction
- Changes in VWF-cleaving Metalloprotease (ADAMTS 13) activity in the thrombotic microangiopathy after kidney tranplantation
- The first successful eculizumab rescue therapy of a kidney transplant recipient with atypical hemolytic uremic syndrome in South Korea: a case report
- Characteristics and management of thrombotic microangiopathy in kidney transplantation
