Electrolyte Blood Press.
2019 Dec;17(2):62-65. 10.5049/EBP.2019.17.2.62.
Severe Hypophosphatemia-Induced Acute Toxic-Metabolic Encephalopathy in Continuous Renal Replacement Therapy
- Affiliations
-
- 1Department of Internal Medicine, Chosun University Medical School, Gwangju, Korea. bcshin@chosun.ac.kr
- KMID: 2467962
- DOI: http://doi.org/10.5049/EBP.2019.17.2.62
Abstract
- Acute toxic-metabolic encephalopathy (TME) is an acute condition of global cerebral dysfunction in the absence of primary structural brain disease. Severe hypophosphatemia leads to muscle weakness and involves the diaphragm but hypophosphatemia-induced TME is very rare. Herein, we report the case of a 43-year-old woman with encephalopathy with severe hypophosphatemia during continuous renal replacement therapy. She presented with features of oliguric acute kidney injury on diabetic kidney disease due to volume depletion. At admission, her mental status was alert but gradually changed to stupor mentation during continuous renal replacement therapy. Her phosphate level was less than 0.41 mEq/L and Glasgow coma scale decreased from 15 to 5. After phosphate intravenous replacement and administration of phosphate-containing replacement solution, the phosphate level increased to 2.97 mEq/L and mental state returned to alert state. This case demonstrates that the level of phosphorus should be observed during continuous renal replacement therapy.
MeSH Terms
Figure
-
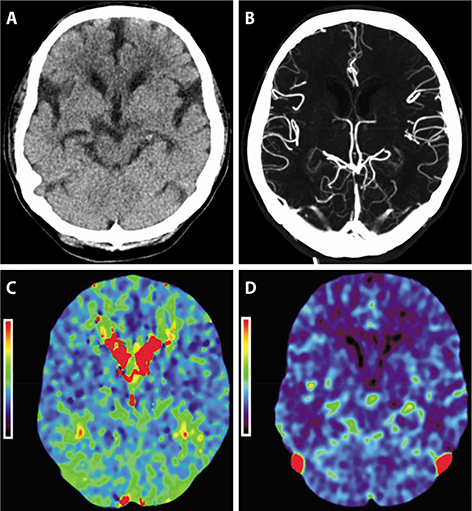
Fig. 1 Brain and neck perfusion CT scan. There were no significant abnormal findings including recent infarction or intracranial hemorrhage, or steno-occlusive lesion (A: non-enhanced CT, B: CT angiography, C, D: perfusion CT angiography).
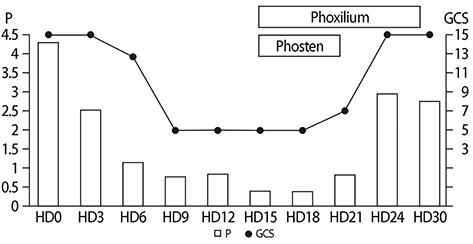
Fig. 2 Serum phosphorus level and Glasgow coma scale follow up. GCS, Glasgow coma scale; P, serum phosphorus level (mEq/L); HD, hospital day.
Reference
-
1. Chen R, Young GB. Metabolic Encephalopathies. In : Bolton CF, Young GB, editors. Baillere's Clinical Neurology. London: Balliere Tindall;p. 577–598.2. Ely EW, Stephens RK, Jackson JC, et al. Current opinions regarding the importance, diagnosis, and management of delirium in the intensive care unit: a survey of 912 healthcare professionals. Crit Care Med. 2004; 32:106–112.
Article3. Young GB, DeRubeis DA. Metabolic encephalopathies. In : Young GB, Ropper AH, Bolton CF, editors. Coma and Impaired Consciousness. McGraw-Hill;1998. p. 307.4. Wijdicks E. Neurologic manifestations of acid base derangements, electrolyte disorders, and endocrine crises. In : Wijdicks E, editor. Neurology of Critical Illness. Philadelphia: FA Davis Company;1995. p. 104.5. Bellomo R, Cass A, Cole L, et al. The relationship between hypophosphataemia and outcomes during low-intensity and high-intensity continuous renal replacement therapy. Crit Care Resusc. 2014; 16:34–41.6. Yang Y, Zhang P, Cui Y, et al. Hypophosphatemia during continuous veno-venous hemofiltration is associated with mortality in critically ill patients with acute kidney injury. Crit Care. 2013; 17:R205.
Article7. Gravelyn TR, Brophy N, Siegert C, et al. Hypophosphatemia-associated respiratory muscle weakness in a general inpatient population. Am J Med. 1998; 84:870–876.
Article8. Kellum JA, Lameire N, Aspelin P, et al. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. 2012; 2:1–138.9. Finkel KW, Podoll AS. Complications of continuous renal replacement therapy. Semin Dial. 2009; 22:155–159.
Article10. Akhoundi A, Singh B, Vela M, et al. Incidence of adverse events during continuous renal replacement therapy. Blood Purif. 2015; 39:333–339.
Article11. Demirjian S, Teo BW, Guzman JA, et al. Hypophosphatemia during continuous hemodialysis is associated with prolonged respiratory failure in patients with acute kidney injury. Nephrol Dial Transplant. 2011; 26:3508–3514.
Article12. Lim C, Tan HK, Kaushik M. Hypophosphatemia in critically ill patients with acute kidney injury treated with hemodialysis is associated with adverse events. Clin Kidney J. 2017; 10:341–347.
Article13. Song YH, Seo EH, Yoo YS, Jo YI. Phosphate supplementation for hypophosphatemia during continuous renal replacement therapy in adults. Ren Fail. 2019; 41:72–79.
Article14. Troyanov S, Geadah D, Ghannoum M, et al. Phosphate addition to hemodiafiltration solutions during continuous renal replacement therapy. Intensive Care Med. 2004; 30:1662–1665.
Article15. Godaly G, Carlsson O, Broman M. Phoxilium(R) reduces hypophosphataemia and magnesium supplementation during continuous renal replacement therapy. Clin Kidney J. 2016; 9:205–210.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The influence of hypophosphatemia on outcomes of low- and high-intensity continuous renal replacement therapy in critically ill patients with acute kidney injury
- Metronidazole Induced Encephalopathy in a Patient with Brain Abscess
- A Case of Diabetic Ketoacidosis with Refractory Metabolic Acidosis Successfully Treated with Continuous Hemodiafiltration
- Continuous Renal Replacement Therapy in Children
- Laundry detergent pod: a rising cause of household poisoning
