A Modified Under-Vastus Approach for Knee Arthroplasty with Anatomical Repair of Soft Tissue
- Affiliations
-
- 1Department of Orthopaedic Surgery and Joint Surgery Centre, Takatsuki General Hospital, Osaka, Japan. takafumi.hiranaka@gmail.com
- KMID: 2462545
- DOI: http://doi.org/10.4055/cios.2019.11.4.490
Abstract
- The under-vastus approach (UVA) is a modification of the conventional subvastus approach for knee arthroplasty. Our modified UVA allows the muscles to be spared while offering good exposure of the operative field and facilitating anatomical repair of the capsule and fascia. A medial parapatellar incision is made and the vastus medialis fascia is incised along the same line. The muscle belly is not incised but detached from the surrounding fascia and retracted laterally. The suprapatellar pouch capsule is then laterally incised under the vastus muscles. The patella can then be easily retracted laterally and adequate exposure is possible. After the procedure, both capsule and fascia can be anatomically repaired. We use this approach for all primary arthroplasties in our practice. There has been no case in which an additional muscle incision was required, and there were no intraoperative complications. The modified UVA allows for excellent exposure of the operative field as well as muscle retention in both primary total and unicompartmental knee arthroplasties.
Keyword
MeSH Terms
Figure
-
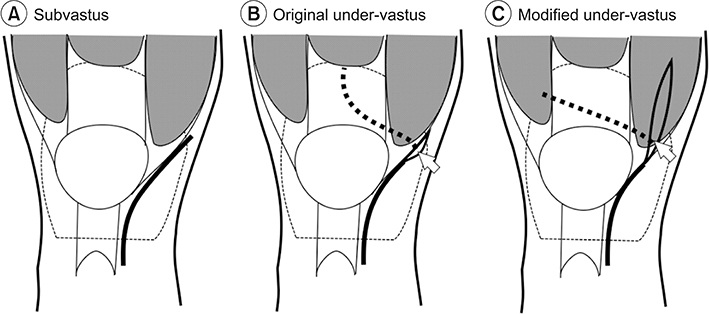
Fig. 1 Line drawing showing the capsule and fascia incisions in three different approaches. Solid lines indicate capsular incision medial to the patella and patellar tendon. The dotted lines indicate capsular incision of suprapatellar pouch under the quadriceps muscle. The arrows indicate where the detachment starts. (A) The conventional subvastus approach. The capsule is cut along the medial border of the patellar tendon and the lower border of the vastus medialis, forming a reversed L shape. (B) The under-vastus approach devised by Tatsumi6). The fascia at the distal end of the vastus medialis is detached and retracted laterally. The capsule of the suprapatellar pouch is incised at the midline. (C) Our modified under-vastus approach. The fascia is incised longitudinally and the muscle belly is retracted laterally. Then, the capsule of the suprapatellar pouch is incised far laterally.
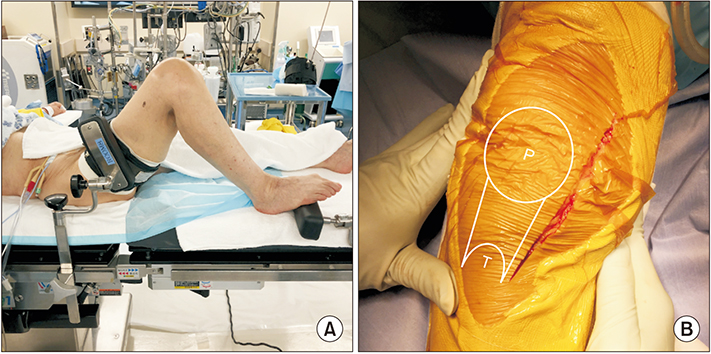
Fig. 2 Leg positioning and skin incision. (A) The operated leg is placed on the table with two-leg supports to maintain the knee flexed to 100°–110°. (B) In the anteromedial aspect of the operated knee, the skin incision is made, starting from 2–3 cm proximal to the superior pole of the patella (P), passing 1–2 cm medial to the patella and the patellar tendon, and ending just medial to the tibial tuberosity (T).
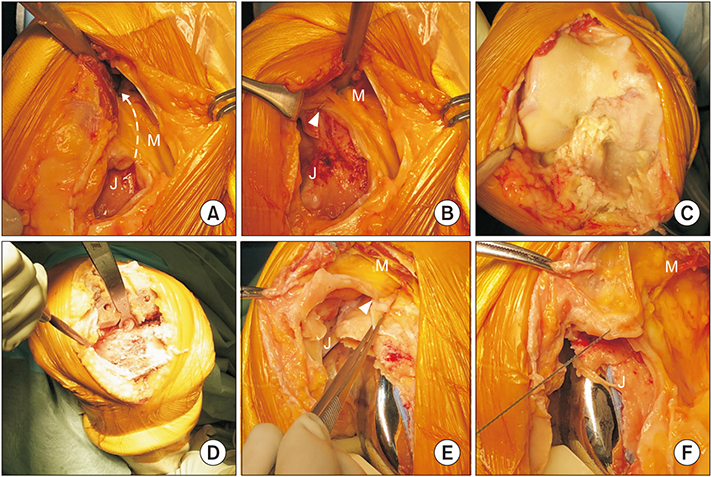
Fig. 3 Surgical steps of the modified under-vastus approach. (A) A capsulotomy is performed under the vastus medialis muscle (broken arrow line). (B) The capsulotomy is complete. The lateral end of the capsulotomy (arrowhead) is visible. (C) Exposure of the femur. Note the muscles are hidden in the skin and are virtually invisible throughout the procedure. (D) Exposure of the tibia. With the posterior and lateral retractors, the tibial cut surface is well exposed. Note the leg is fully flexed by the assistant. (E) At closure, a continuous suture is started at the lateral end of the capsulotomy (arrowhead). (F) The capsule of the suprapatellar pouch is sutured. J: joint cavity of the knee, M: vastus medialis muscle and its compartment.
Reference
-
1. Hofmann AA, Plaster RL, Murdock LE. Subvastus (Southern) approach for primary total knee arthroplasty. Clin Orthop Relat Res. 1991; (269):70–77.
Article2. Roysam GS, Oakley MJ. Subvastus approach for total knee arthroplasty: a prospective, randomized, and observer-blinded trial. J Arthroplasty. 2001; 16(4):454–457.3. Scuderi GR, Tenholder M, Capeci C. Surgical approaches in mini-incision total knee arthroplasty. Clin Orthop Relat Res. 2004; (428):61–67.
Article4. Tria AJ Jr, Coon TM. Minimal incision total knee arthroplasty: early experience. Clin Orthop Relat Res. 2003; (416):185–190.
Article5. Boerger TO, Aglietti P, Mondanelli N, Sensi L. Mini-subvastus versus medial parapatellar approach in total knee arthroplasty. Clin Orthop Relat Res. 2005; 440:82–87.
Article6. Tatsumi I. Under vastus approach MIS-TKA. J Minim Invasive Orthop Surg. 2010; 54:75–82.7. Matsueda M, Gustilo RB. Subvastus and medial parapatellar approaches in total knee arthroplasty. Clin Orthop Relat Res. 2000; (371):161–168.
Article8. Gore DR, Sellinger DS, Gassner KJ, Glaeser ST. Subvastus approach for total knee arthroplasty. Orthopedics. 2003; 26(1):33–35.
Article9. Teng Y, Du W, Jiang J, et al. Subvastus versus medial parapatellar approach in total knee arthroplasty: meta-analysis. Orthopedics. 2012; 35(12):e1722–e1731.
Article10. Ritter MA, Pierce MJ, Zhou H, Meding JB, Faris PM, Keating EM. Patellar complications (total knee arthroplasty): effect of lateral release and thickness. Clin Orthop Relat Res. 1999; (367):149–157.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Total Knee Arthroplasty Using Tissue Expander In Patient with Poor Soft Tissue Coverage of Knee: A Case Report
- Modified Medial Gastrocnemius Myocutaneous Flap Technique for Knee Joint Coverage after Total Knee Arthroplasty
- Treatment of Soft Tissue Defect after TKA Using Dorsalis Pedis Flap: A Case Report
- Modified Posterior Approach to Total Hip Arthroplasty
- The Comparision of the Midvastus and Paramedian Approaches for Total Knee Arthroplasty
