Full mouth rehabilitation in a patient with peri-implantitis: A case report
- Affiliations
-
- 1Department of Prosthodontics, School of Medicine, Ewha Womans University, Seoul, Republic of Korea. prosth@ewha.ac.kr
- KMID: 2461149
- DOI: http://doi.org/10.4047/jkap.2019.57.4.416
Abstract
- Peri-implantitis appears in almost 20% of patients who received implant treatment, and increase in its number is inevitable as time goes by. Although it can be treated by both non-surgical and surgical procedures, in cases which include severe bone loss, explantation and rehabilitation may be necessary. Careful treatment planning and considerations to prevent recurrent peri-implantitis should be taken into account. In the following case presented, a patient with chronic periodontitis and peri-implantitis was successfully rehabilitated after removal of several implants. Extraction and explantation of multiple teeth and implants were followed by full mouth reconstruction with fixed implant prostheses on the mandible and implant retained overdenture on the maxilla. Surgical and prosthetic measures to prevent recurrent peri-implantitis were taken into consideration.
Keyword
MeSH Terms
Figure
-
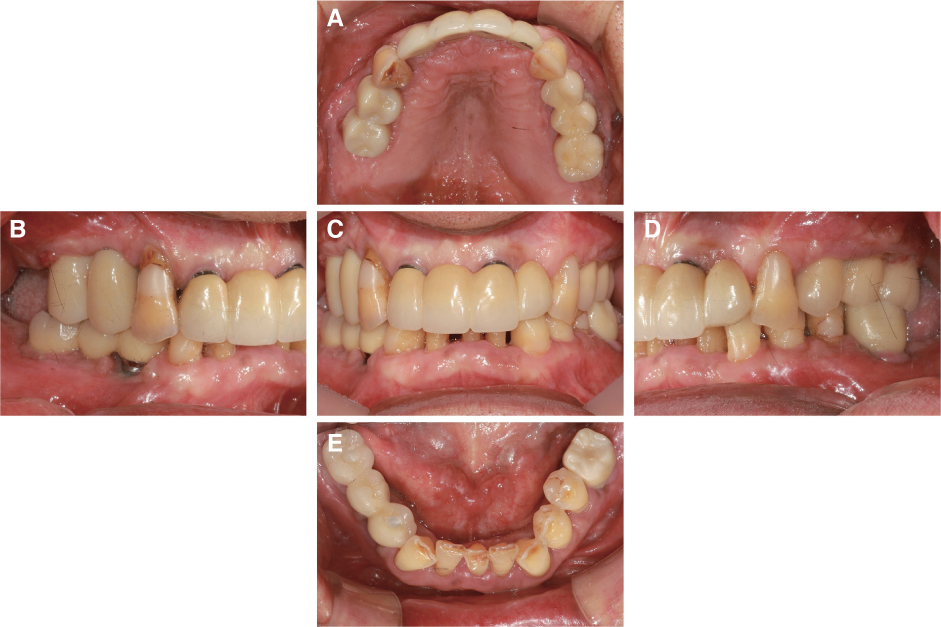
Fig. 1 Pre-operative intraoral view (A – E). (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.
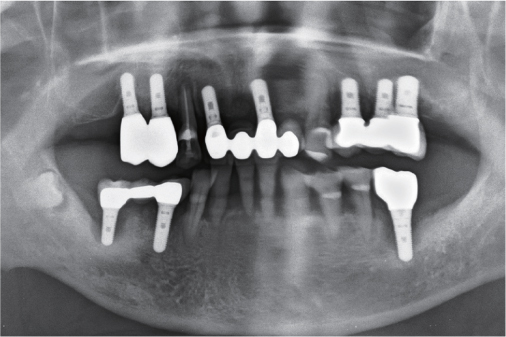
Fig. 2 Pre-operative panoramic X-ray showing generalized alveolar bone loss.

Fig. 3 Diagnostic wax-up and arrangement on diagnostic model. (A) Right lateral view, (B) Fontal view, (C) Left lateral view.

Fig. 4 Provisional restorations. (A) Right lateral view, (B) Frontal view, (C) Left lateral view (Yellow arrow shows less interproximal space under provisional restorations).
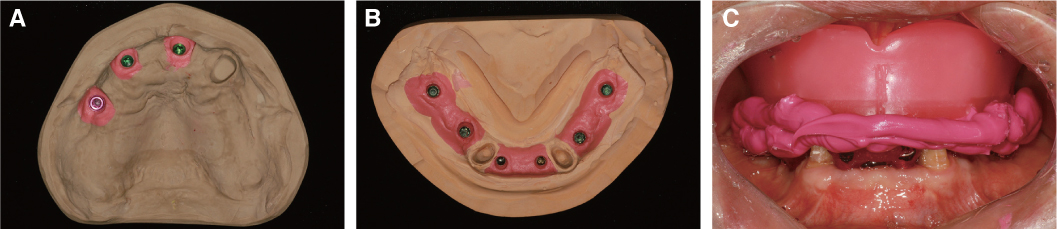
Fig. 5 Prosthetic process for final restorations. (A) Master cast of maxilla, (B) Master cast of mandible, (C) Bite registration with wax-rim on maxilla and fixed bite jig on mandible, fabricated with titanium temporary cylinders and pattern resin.

Fig. 6 (A) Computer-aided design of final restorations, (B) Computer-aided design of custom abutments, (C) Try-in of custom abutments.

Fig. 7 Fabricated final restorations. (A) Right lateral view, (B) Frontal view, (C) Left lateral view. Over-contour was minimized and sufficient interproximal spaces were provided.
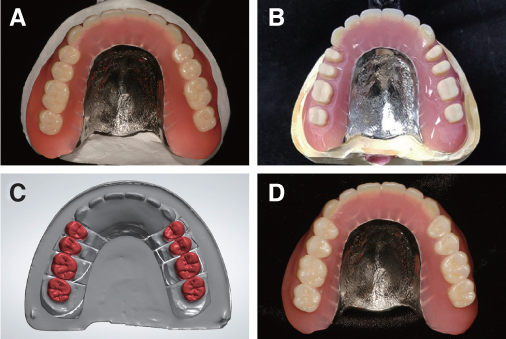
Fig. 8 (A) Conventionally cured maxillary denture, (B) Preparation of denture teeth (premolars and molars), (C) Computer-aided design of zirconia crowns, (D) Final maxillary denture with zirconia crowns on premolars and molars for additional resistance from attrition by antagonistic mandibular zirconia restorations.
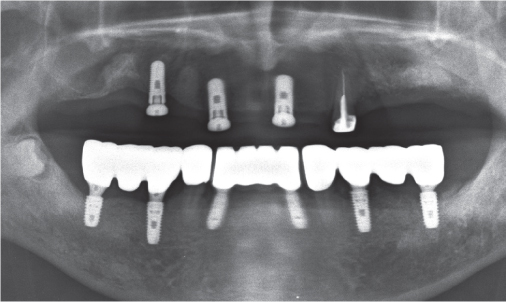
Fig. 9 Panoramic X-ray after mandibular prostheses delivery.
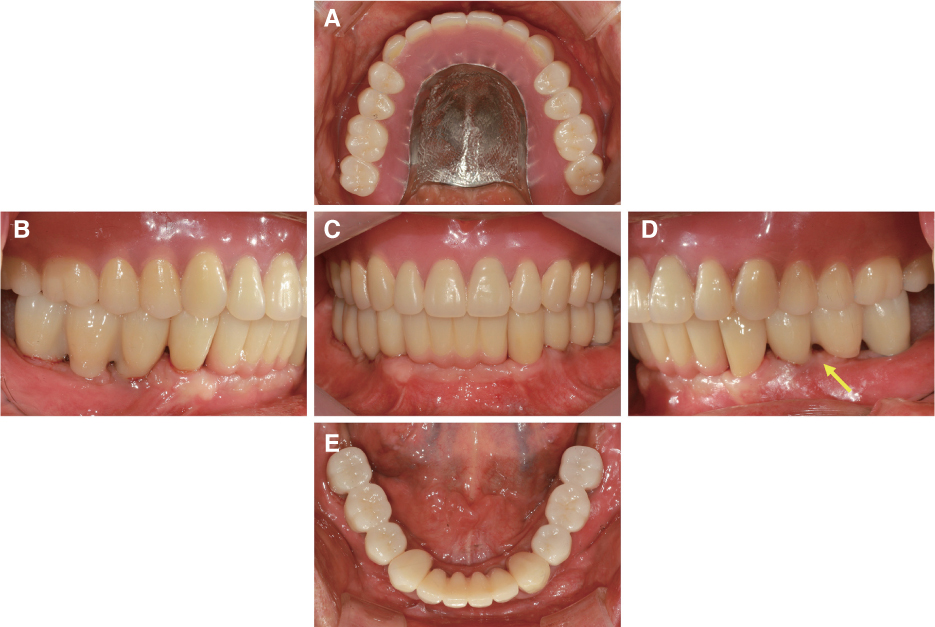
Fig. 10 Definitive restorations (A – E). (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view (Yellow arrow shows adequate interproximal space under definitive restorations).
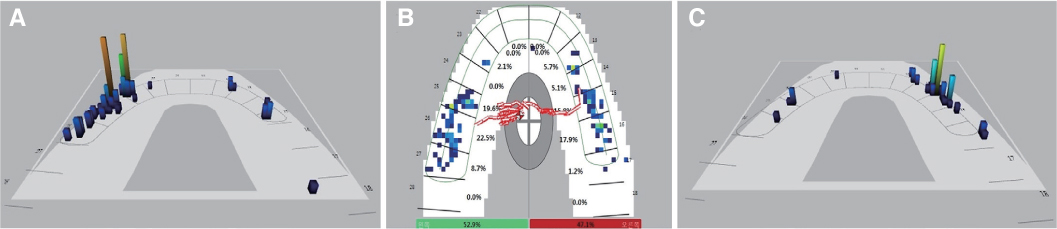
Fig. 11 T-Scan of definitive prostheses showing bilaterally balanced occlusion. (A) Left lateral movement of mandible, (B) Maximum intercuspation, (C) Right lateral movement of mandible.
Reference
-
1. Mombelli A, Müller N, Cionca N. The epidemiology of peri-implantitis. Clin Oral Implants Res. 2012; 23 Supple 6:67–76.
Article2. Lindhe J, Meyle J;. Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:282–285.
Article3. Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol. 2008; 35:292–304.
Article4. Karoussis IK, Salvi GE, Heitz-Mayfield LJ, Brägger U, Hämmerle CH, Lang NP. Long-term implant prognosis in patients with and without a history of chronic periodontitis: a 10-year prospective cohort study of the ITI Dental Implant System. Clin Oral Implants Res. 2003; 14:329–339.
Article5. Lang NP, Wilson TG, Corbet EF. Biological complications with dental implants: their prevention, diagnosis and treatment. Clin Oral Implants Res. 2000; 11:146–155.
Article6. Tallarico M, Canullo L, Wang HL, Cochran DL, Meloni SM. Classification systems for peri-implantitis: A narrative review with a proposal of a new evidence-based etiology codification. Int J Oral Maxillofac Implants. 2018; 33:871–879.
Article7. Naert I, Duyck J, Vandamme K. Occlusal overload and bone/implant loss. Clin Oral Implants Res. 2012; 23:95–107.
Article8. Lee CT, Huang YW, Zhu L, Weltman R. Prevalences of periimplantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent. 2017; 62:1–12.
Article9. Kotsovilis S, Karoussis IK, Trianti M, Fourmousis I. Therapy of peri-implantitis: a systematic review. J Clin Periodontol. 2008; 35:621–629.
Article10. Jepsen S, Berglundh T, Genco R, Aass AM, Demirel K, Derks J, Figuero E, Giovannoli JL, Goldstein M, Lambert F, Ortiz-Vigon A, Polyzois I, Salvi GE, Schwarz F, Serino G, Tomasi C, Zitzmann NU. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol. 2015; 42:S152–S157.
Article11. Schou S, Berglundh T, Lang NP. Surgical treatment of periimplantitis. Int J Oral Maxillofac Implants. 2004; 19:140–149.12. Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis evidence for a microbial cause of peri-implant infections. Periodontology. 2000; 17:63–76.13. Ding L, Zhang P, Wang X, Kasugai S. A doxycycline-treated hydroxyapatite implant surface attenuates the progression of peri-implantitis: A radiographic and histological study in mice. Clin Implant Dent Relat Res. 2019; 21:154–159.
Article14. Becker W, Becker BE, Newman MG, Nyman S. Clinical and microbiologic findings that may contribute to dental implant failure. Int J Oral Maxillofac Implants. 1990; 5:31–38.15. Ozeki K, Okuyama Y, Fukui Y, Aoki H. Bone response to titanium implants coated with thin sputtered HA film subject to hydrothermal treatment and implanted in the canine mandible. Biomed Mater Eng. 2006; 16:243–251.16. Roos-Jansåker AM, Renvert H, Lindahl C, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part III: factors associated with peri-implant lesions. J Clin Periodontol. 2006; 33:296–301.
Article17. Salvi GE, Monje A, Tomasi C. Long-term biological complications of dental implants placed either in pristine or in augmented sites: A systematic review and meta-analysis. Clin Oral Implants Res. 2018; 29:294–310.
Article18. Bremer F, Grade S, Kohorst P, Stiesch M. In vivo biofilm formation on different dental ceramics. Quintessence Int. 2011; 42:565–574.19. Katafuchi M, Weinstein BF, Leroux BG, Chen YW, Daubert DM. Restoration contour is a risk indicator for peri-implantitis: A cross-sectional radiographic analysis. J Clin Periodontol. 2018; 45:225–232.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk factors of peri-implantitis: a narrative review
- Unusual bone regeneration following resective surgery and decontamination of peri-implantitis: a 6-year follow-up
- Management of peri-implantitis associated with tear-like implant fracture: case reports
- Laser therapy in peri-implantitis treatment: literature review
- Prevalence and risk factors of peri-implantitis: A retrospective study
