Left Atrial Function Following Surgical Ablation of Atrial Fibrillation: Prospective Evaluation Using Dual-Source Cardiac Computed Tomography
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jwlee@amc.seoul.kr
- 2Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2450332
- DOI: http://doi.org/10.3349/ymj.2015.56.3.608
Abstract
- PURPOSE
The Maze procedure has shown excellent efficacy in the elimination of atrial fibrillation (AF); however, little is known about the quality of functional recovery in the left atrium (LA) following successful sinus rhythm conversion by the Maze procedure.
MATERIALS AND METHODS
We prospectively enrolled 12 patients (aged 52.5+/-10.1 years, 1 female) with valvular AF undergoing mitral valve surgery combined with the Maze procedure. Parameters of LA function in three anatomic compartments [anterior, posterior, and LA appendage (LAA)] were evaluated using electrocardiography-gated dual-source cardiac CT at one month and at six months after surgery. Twelve subjects matched by age, gender, and body surface area served as controls.
RESULTS
At one month after surgery, ejection fraction (EF) and emptying volume (EV) of the LA were 14.9+/-7.4% and 21.3+/-9.7 mL, respectively, and they were significantly lower than those of the control group (EF, 47.9+/-11.2%; EV, 46.0+/-10.7%; p<0001). These values did not significantly change throughout late periods (p=0.22 and 0.21, respectively). Functional contributions of the anterior, posterior, and appendage compartments (EV of each compartment/overall EV) were 80.4%, -0.9%, and 20.5%, respectively, for those with LAA preservation (n=6); 100.1%, -0.1%, and 0% for those with LAA resection (n=6; p<0.05); and 62.2%, 28.2%, and 9.7% in the control subjects (p<0.001).
CONCLUSION
Contractile functions of the LA significantly decreased after the Maze procedure. Functional contributions of three compartments of the LA were also altered. The influence of LAA preservation on postoperative LA functions needs to be evaluated through studies of larger populations.
MeSH Terms
Figure
-
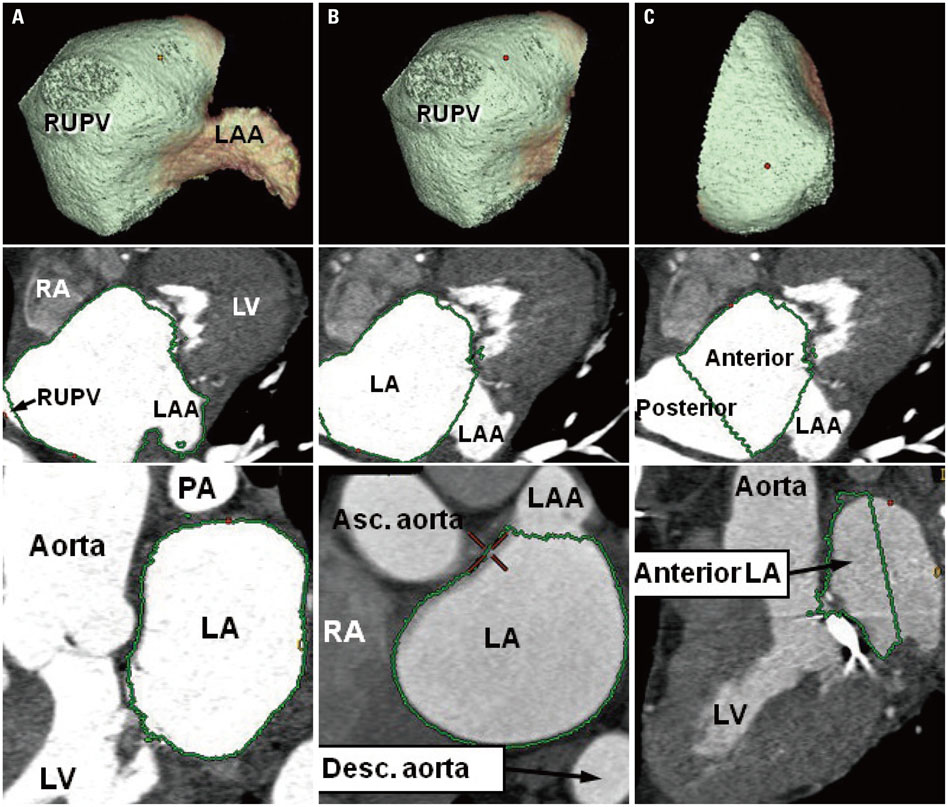
Fig. 1 Three-dimensional measurement of LA volumes using volume-rendering imaging. Green demarcation lines indicate the extents of measurement for each compartment including (A), entire LA (right-anterior view); (B) LAA-extracted LA (right-anterior view); and (C) anterior compartment of the LA (right lateral view). RUPV, right upper pulmonary vein; LA, left atrium; LAA, left atrial appendage; RA, right atrium; LV, left ventricle; PA, pulmonary artery.

Fig. 2 Changes in overall LA volume at each time point. (A) Maximal volumes. (B) Minimal volume. LA, left atrium; LAA, left atrial appendage.

Fig. 3 LA contractile function at one and six months after surgery. (A) LA emptying volume. (B) LA ejection fraction. LA, left atrium; LAA, left atrial appendage.
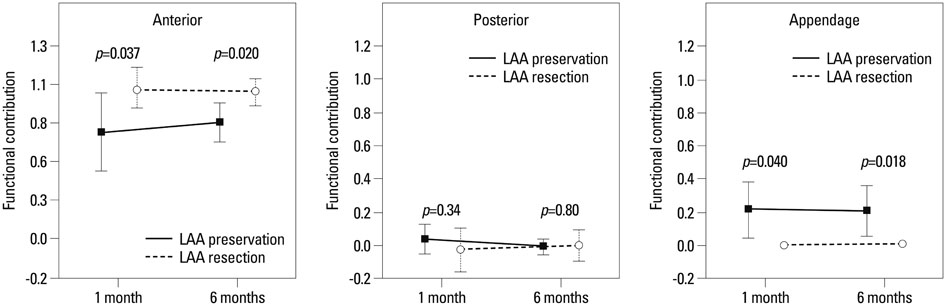
Fig. 4 Booster functional contribution of each left atrial chamber (anterior, posterior, and LAA) at one and six months after surgery. LAA, left atrial appendage.
Cited by 1 articles
-
Clinical Significance of Additional Ablation of Atrial Premature Beats after Catheter Ablation for Atrial Fibrillation
In-Soo Kim, Pil-Sung Yang, Tae-Hoon Kim, Junbeum Park, Jin-Kyu Park, Jae Sun Uhm, Boyoung Joung, Moon Hyoung Lee, Hui-Nam Pak
Yonsei Med J. 2016;57(1):72-80. doi: 10.3349/ymj.2016.57.1.72.
Reference
-
1. Ad N, Henry L, Hunt S. The impact of surgical ablation in patients with low ejection fraction, heart failure, and atrial fibrillation. Eur J Cardiothorac Surg. 2011; 40:70–76.
Article2. Bando K, Kasegawa H, Okada Y, Kobayashi J, Kada A, Shimokawa T, et al. Impact of preoperative and postoperative atrial fibrillation on outcome after mitral valvuloplasty for nonischemic mitral regurgitation. J Thorac Cardiovasc Surg. 2005; 129:1032–1040.
Article3. Cohn LH, Couper GS, Aranki SF, Rizzo RJ, Kinchla NM, Collins JJ Jr. Long-term results of mitral valve reconstruction for regurgitation of the myxomatous mitral valve. J Thorac Cardiovasc Surg. 1994; 107:143–150.
Article4. Cox JL, Ad N, Palazzo T. Impact of the maze procedure on the stroke rate in patients with atrial fibrillation. J Thorac Cardiovasc Surg. 1999; 118:833–840.
Article5. Cox JL, Boineau JP, Schuessler RB, Ferguson TB Jr, Cain ME, Lindsay BD, et al. Successful surgical treatment of atrial fibrillation. Review and clinical update. JAMA. 1991; 266:1976–1980.
Article6. Gillinov AM, Sirak J, Blackstone EH, McCarthy PM, Rajeswaran J, Pettersson G, et al. The Cox maze procedure in mitral valve disease: predictors of recurrent atrial fibrillation. J Thorac Cardiovasc Surg. 2005; 130:1653–1660.
Article7. Kim JB, Moon JS, Yun SC, Kim WK, Jung SH, Choo SJ, et al. Long-term outcomes of mechanical valve replacement in patients with atrial fibrillation: impact of the maze procedure. Circulation. 2012; 125:2071–2080.
Article8. Park MJ, Jung JI, Oh YS, Youn HJ. Assessment of the structural remodeling of the left atrium by 64-multislice cardiac CT: comparative studies in controls and patients with atrial fibrillation. Int J Cardiol. 2012; 159:181–186.
Article9. Yamanaka K, Fujita M, Doi K, Tsuneyoshi H, Yamazato A, Ueno K, et al. Multislice computed tomography accurately quantifies left atrial size and function after the MAZE procedure. Circulation. 2006; 114:1 Suppl. I5–I9.
Article10. den Uijl DW, Tops LF, Delgado V, Schuijf JD, Kroft LJ, de Roos A, et al. Effect of pulmonary vein anatomy and left atrial dimensions on outcome of circumferential radiofrequency catheter ablation for atrial fibrillation. Am J Cardiol. 2011; 107:243–249.
Article11. Kataoka A, Funabashi N, Takahashi A, Yajima R, Takahashi M, Uehara M, et al. Quantitative evaluation of left atrial volumes and ejection fraction by 320-slice computed-tomography in comparison with three- and two-dimensional echocardiography: a single-center retrospective-study in 22 subjects. Int J Cardiol. 2011; 153:47–54.
Article12. Kim JB, Bang JH, Jung SH, Choo SJ, Chung CH, Lee JW. Left atrial ablation versus biatrial ablation in the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2011; 92:1397–1404.
Article13. Kerut EK. Anatomy of the left atrial appendage. Echocardiography. 2008; 25:669–673.
Article14. Abhayaratna WP, Seward JB, Appleton CP, Douglas PS, Oh JK, Tajik AJ, et al. Left atrial size: physiologic determinants and clinical applications. J Am Coll Cardiol. 2006; 47:2357–2363.15. Middlekauff HR, Stevenson WG, Stevenson LW. Prognostic significance of atrial fibrillation in advanced heart failure. A study of 390 patients. Circulation. 1991; 84:40–48.
Article16. Pritchett EL. Management of atrial fibrillation. N Engl J Med. 1992; 326:1264–1271.
Article17. Feinberg MS, Waggoner AD, Kater KM, Cox JL, Lindsay BD, Pérez JE. Restoration of atrial function after the maze procedure for patients with atrial fibrillation. Assessment by Doppler echocardiography. Circulation. 1994; 90(5 Pt 2):II285–II292.18. Yashima N, Nasu M, Kawazoe K, Hiramori K. Serial evaluation of atrial function by Doppler echocardiography after the maze procedure for chronic atrial fibrillation. Eur Heart J. 1997; 18:496–502.
Article19. Jessurun ER, van Hemel NM, Kelder JC, Defauw JA, Brutel de la Rivière A, Ernst JM, et al. The effect of maze operations on atrial volume. Ann Thorac Surg. 2003; 75:51–56.
Article20. Anderson RH, Cook AC. The structure and components of the atrial chambers. Europace. 2007; 9:Suppl 6. vi3–vi9.
Article21. Cox JL. The central controversy surrounding the interventional-surgical treatment of atrial fibrillation. J Thorac Cardiovasc Surg. 2005; 129:1–4.
Article22. Lönnerholm S, Blomström P, Nilsson L, Oxelbark S, Jideus L, Blomström-Lundqvist C. Effects of the maze operation on health-related quality of life in patients with atrial fibrillation. Circulation. 2000; 101:2607–2611.
Article23. Henry WL, Morganroth J, Pearlman AS, Clark CE, Redwood DR, Itscoitz SB, et al. Relation between echocardiographically determined left atrial size and atrial fibrillation. Circulation. 1976; 53:273–279.
Article24. Bailey GW, Braniff BA, Hancock EW, Cohn KE. Relation of left atrial pathology to atrial fibrillation in mitral valvular disease. Ann Intern Med. 1968; 69:13–20.
Article25. Lin WS, Tai CT, Hsieh MH, Tsai CF, Lin YK, Tsao HM, et al. Catheter ablation of paroxysmal atrial fibrillation initiated by non-pulmonary vein ectopy. Circulation. 2003; 107:3176–3183.
Article26. Shinbane JS, Wood MA, Jensen DN, Ellenbogen KA, Fitzpatrick AP, Scheinman MM. Tachycardia-induced cardiomyopathy: a review of animal models and clinical studies. J Am Coll Cardiol. 1997; 29:709–715.
Article27. Umana E, Solares CA, Alpert MA. Tachycardia-induced cardiomyopathy. Am J Med. 2003; 114:51–55.
Article28. Stulak JM, Dearani JA, Daly RC, Zehr KJ, Sundt TM 3rd, Schaff HV. Left ventricular dysfunction in atrial fibrillation: restoration of sinus rhythm by the Cox-maze procedure significantly improves systolic function and functional status. Ann Thorac Surg. 2006; 82:494–500.
Article29. Nedios S, Sommer P, Dagres N, Kosiuk J, Arya A, Richter S, et al. Long-term follow-up after atrial fibrillation ablation in patients with impaired left ventricular systolic function: the importance of rhythm and rate control. Heart Rhythm. 2014; 11:344–351.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Underdevelopment of Left Atrial Appendage
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Relationship between Epicardial Fat Accumulation and Left Atrial Reverse Remodeling after Catheter Ablation of Atrial Fibrillation
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
- A Totally Thoracoscopic Ablation for Persistent Atrial Fibrillation
