Analysis of Inner Ear Anomalies in Unilateral Congenital Aural Atresia Combined With Microtia
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Korea University College of Medicine, Seoul, Korea. logopas@korea.ac.kr
- KMID: 2447426
- DOI: http://doi.org/10.21053/ceo.2018.00857
Abstract
OBJECTIVES
The aim of this study was to analyze the incidence of inner ear anomalies in patients with unilateral congenital aural atresia (CAA) combined with microtia.
METHODS
We retrospectively reviewed 61 patients with unilateral CAA combined with microtia who underwent high-resolution temporal bone computed tomography (TBCT) and hearing examination. Inner ear anomalies were analyzed using TBCT and evaluated according to the Jahrsdoerfer grading system, Marx classification, and extent of inferior displacement of the mastoid tegmen.
RESULTS
Inner ear anomalies were observed in 14 patients (23.0%). Lateral semicircular canal (LSCC) dysplasia was the most common inner ear anomaly, with an incidence of 16.4%. The incidence was significantly higher on the pathologic side than on the unaffected side (P=0.002). All vascular anomalies were observed in the high-riding jugular bulb, with an incidence of 24.6%. The incidence was significantly higher on the pathologic side than on the unaffected side (P<0.001). LSCC dysplasia was significantly more common in patients with a lower Jahrsdoerfer score (odds ratio, 0.66; P=0.004).
CONCLUSION
The incidence of inner ear anomalies was relatively high in patients with unilateral CAA combined with microtia; LSCC dysplasia was the most common anomaly and the probability of coexistence was higher in patients with a lower Jahrsdoerfer score.
MeSH Terms
Figure
-
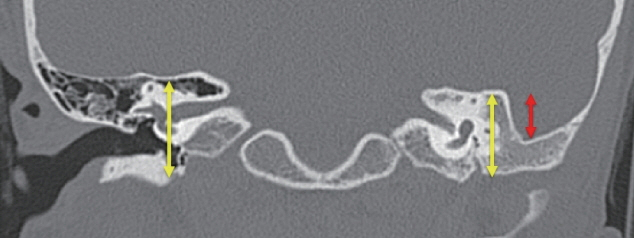
Fig. 1. The extent of inferior displacement of the mastoid tegmen was calculated as the ratio of middle ear height to mastoid tegmen displacement (yellow arrows, middle ear height; red arrow, mastoid tegmen displacement).
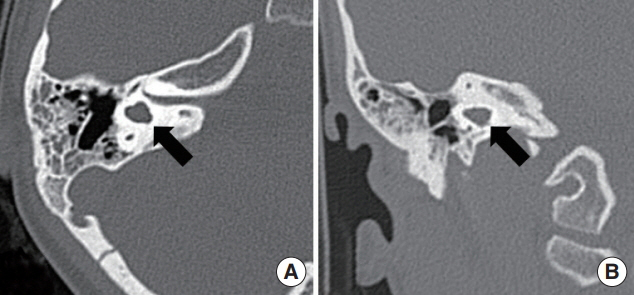
Fig. 2. High-resolution temporal bone computed tomography images of unilateral congenital aural atresia combined with microtia. Axial (A) and coronal (B) views showing the dysmorphic features of the lateral semicircular canal (arrows).
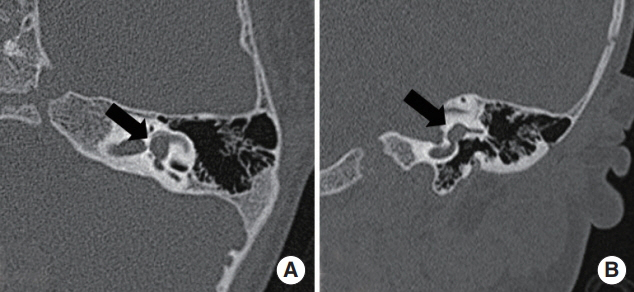
Fig. 3. High-resolution temporal bone computed tomography images of unilateral congenital aural atresia combined with microtia. Axial (A) and coronal (B) views showing the dilated vestibular morphology (arrows).
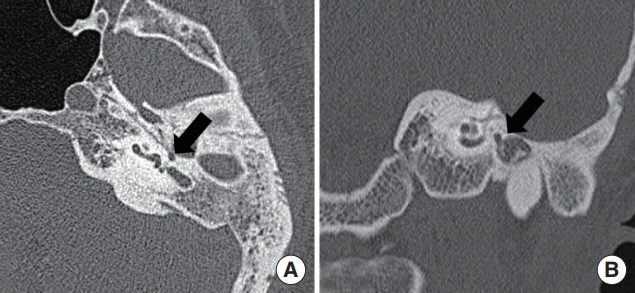
Fig. 4. High-resolution temporal bone computed tomography images of unilateral congenital aural atresia combined with microtia. Axial (A) and coronal (B) views showing the medio-inferiorly displaced tympanic segment of the facial nerve (arrows).

Fig. 5. High-resolution temporal bone computed tomography images of unilateral congenital aural atresia combined with microtia. Axial (A) and coronal (B) views showing high-riding jugular bulb (arrows).
Cited by 1 articles
-
Increased Risk of Psychopathological Abnormalities in Subjects With Unilateral Hearing Loss: A Cross-Sectional Study
Jae-Jin Song, Eu Jeong Ku, Seoyoung Kim, Euitae Kim, Young-Seok Choi, Hahn Jin Jung
Clin Exp Otorhinolaryngol. 2021;14(1):82-87. doi: 10.21053/ceo.2020.00283.
Reference
-
1. Schuknecht HF. Congenital aural atresia. Laryngoscope. 1989; Sep. 99(9):908–17.
Article2. Genc S, Kahraman E, Ozel HE, Arslan IB, Demir A, Selcuk A. Microtia and congenital aural atresia. J Craniofac Surg. 2012; Nov. 23(6):1733–5.
Article3. Vrabec JT, Lin JW. Inner ear anomalies in congenital aural atresia. Otol Neurotol. 2010; Dec. 31(9):1421–6.
Article4. Mayer TE, Brueckmann H, Siegert R, Witt A, Weerda H. High-resolution CT of the temporal bone in dysplasia of the auricle and external auditory canal. AJNR Am J Neuroradiol. 1997; Jan. 18(1):53–65.5. Yuen HY, Ahuja AT, Wong KT, Yue V, van Hasselt AC. Computed tomography of common congenital lesions of the temporal bone. Clin Radiol. 2003; Sep. 58(9):687–93.
Article6. Naunton RF, Valvassori GE. Inner ear anomalies: their association with atresia. Laryngoscope. 1968; Jun. 78(6):1041–9.
Article7. Phelps PD. Congenital lesions of the inner ear, demonstrated by tomography. Arch Otolaryngol. 1974; Jul. 100(1):11–8.8. Halle TR, Soares BP, Todd NW. Inner ear anomalies in children with isolated unilateral congenital aural atresia. Int J Pediatr Otorhinolaryngol. 2017; Apr. 95:5–8.
Article9. Balaker AE, Roberson JB Jr, Goldsztein H. Fibrous incudostapedial joint in congenital aural atresia. Otolaryngol Head Neck Surg. 2014; Apr. 150(4):673–6.
Article10. Yellon RF, Branstetter BF 4th. Prospective blinded study of computed tomography in congenital aural atresia. Int J Pediatr Otorhinolaryngol. 2010; Nov. 74(11):1286–91.
Article11. Jahrsdoerfer RA, Yeakley JW, Aguilar EA, Cole RR, Gray LC. Grading system for the selection of patients with congenital aural atresia. Am J Otol. 1992; Jan. 13(1):6–12.
Article12. Dedhia K, Yellon RF, Branstetter BF, Egloff AM. Anatomic variants on computed tomography in congenital aural atresia. Otolaryngol Head Neck Surg. 2012; Aug. 147(2):323–8.
Article13. Kim DW, Lee JH, Song JJ, Chang H, Choi YS, Jang JH, et al. Continuity of the incudostapedial joint: a novel prognostic factor in postoperative hearing outcomes in congenital aural atresia. Acta Otolaryngol. 2011; Jul. 131(7):701–7.
Article14. Ju YH, Park E, Park S, Jung K, Lee K, Im GJ. The extent of inferior displacement of the mastoid tegmen is related to the severity of congenital aural atresia. Acta Otolaryngol. 2014; Mar. 134(3):244–9.
Article15. Sennaroglu L, Saatci I. A new classification for cochleovestibular malformations. Laryngoscope. 2002; Dec. 112(12):2230–41.
Article16. Brook CD, Buch K, Kaufmann M, Sakai O, Devaiah AK. The prevalence of high-riding jugular bulb in patients with suspected endolymphatic hydrops. J Neurol Surg B Skull Base. 2015; Dec. 76(6):471–4.17. Frenzel H, Sprinzl G, Widmann G, Petersen D, Wollenberg B, Mohr C. Grading system for the selection of patients with congenital aural atresia for active middle ear implants. Neuroradiology. 2013; Jul. 55(7):895–911.
Article18. Yu Z, Han D, Gong S, Wang Z, Dai H, Zhao S, et al. Facial nerve course in congenital aural atresia: identified by preoperative CT scanning and surgical findings. Acta Otolaryngol. 2008; 128(12):1375–80.19. Takegoshi H, Kaga K, Kikuchi S, Ito K. Facial canal anatomy in patients with microtia: evaluation of the temporal bones with thin-section CT. Radiology. 2002; Dec. 225(3):852–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Proximal 16p11.2 Deletion in a Term Infant with Unilateral Microtia and Aural Atresia: A Case Report
- Functional and esthetic reconstruction of microtia and congenital aural atresia: a case report
- Management of Congenital Aural Atresia and Microtia
- Clinical Analysis of Neonatal Microtia
- Congenital Aural Atresia Associated with Cholesteatoma
