Qualitative and Quantitative Comparison of Contrast-Enhanced Fluid-Attenuated Inversion Recovery, Magnetization Transfer Spin Echo, and Fat-Saturation T1-Weighted Sequences in Infectious Meningitis
- Affiliations
-
- 1Department of Radiology, SGRR Institute of Medical & Health Sciences, Patel Nagar, Dehradun 248001, India. rajivas23@yahoo.com
- 2Department of Pathology, SGRR Institute of Medical & Health Sciences, Patel Nagar, Dehradun 248001, India.
- KMID: 2427207
- DOI: http://doi.org/10.3348/kjr.2017.18.6.973
Abstract
OBJECTIVE
To compare the contrast-enhanced fluid-attenuated inversion recovery (CE-FLAIR), the CE T1-weighted (CE-T1W) sequence with fat suppression (FS) and magnetization transfer (MT) for early detection and characterization of infectious meningitis.
MATERIALS AND METHODS
Fifty patients and 10 control subjects were evaluated with the CE-FLAIR and the CE-T1W sequences with FS and MT. Qualitative assessment was done by two observers for presence and grading of abnormal leptomeningeal enhancement. Quantitative assessment included computation of net meningeal enhancement, using single pixel signal intensity software. A newly devised FLAIR based scoring system, based on certain imaging features including ventricular dilatation, ependymal enhancement, infarcts and subdural effusions was used to indicate the etiology. Data were analysed using the Student's t test, Cohen's Kappa coefficient, Pearson's correlation coefficient, the intraclass correlation coefficient, one way analysis of variance, and Fisher's exact test with Bonferroni correction as the post hoc test.
RESULTS
The CE-FLAIR sequence demonstrated a better sensitivity (100%), diagnostic accuracy (95%), and a stronger correlation with the cerebrospinal fluid, total leukocyte count (r = 0.75), protein (r = 0.77), adenosine deaminase (r = 0.81) and blood glucose (r = -0.6) values compared to the CE-T1W sequences. Qualitative grades and quantitative meningeal enhancement on the CE-FLAIR sequence were also significantly greater than those on the other sequences. The FLAIR based scoring system yielded a diagnostic accuracy of 91.6% and a sensitivity of 96%. A strong inverse Pearson's correlation (r = -0.95) was found between the assigned score and patient's Glasgow Coma Scale at the time of admission.
CONCLUSION
The CE-FLAIR sequence is better suited for evaluating infectious meningitis and could be included as a part of the routine MR imaging protocol.
Keyword
MeSH Terms
-
Adenosine Deaminase/cerebrospinal fluid
Adolescent
Adult
Aged
Aged, 80 and over
Blood Glucose/analysis
Child
Child, Preschool
Contrast Media/chemistry
Female
Humans
Leukocyte Count
Magnetic Resonance Imaging/*methods
Male
Meningitis/*diagnosis
Middle Aged
Sensitivity and Specificity
Young Adult
Blood Glucose
Contrast Media
Adenosine Deaminase
Figure
-
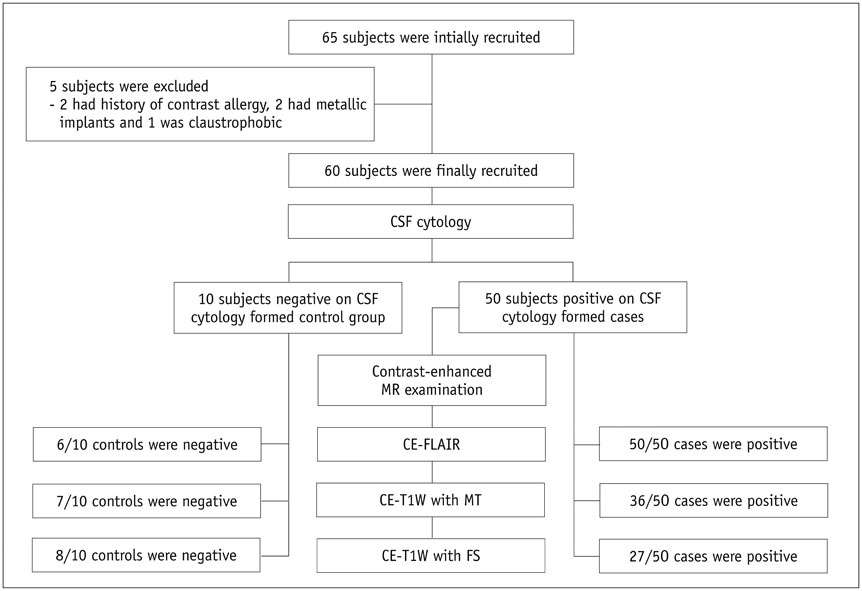
Fig. 1 Flow diagram depicting recruitment of subjects and study design following STARD guidelines. CE-FLAIR = contrast-enhanced fluid-attenuated inversion recovery, CE-T1W = contrast-enhanced T1-weighted, CSF = cerebrospinal fluid, FS = fat suppression, MT = magnetization transfer
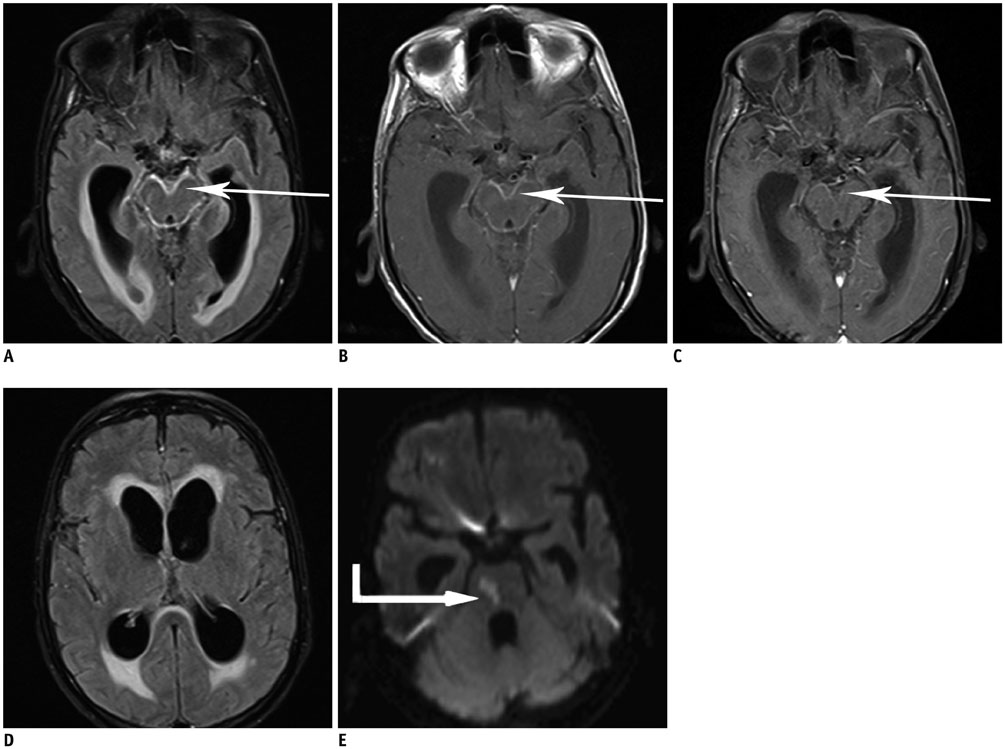
Fig. 2 MR imaging in 75-year-old male with tubercular meningitis. CE-FLAIR (A, D) CE-T1W with MT (B), CE-T1W with FS images (C), DWI (E) depict grade 3 meningeal enhancement on CE-FLAIR sequence (arrows), compared to only grade 2 and grade 1 enhancement on CE-T1W sequences with MT and FS, respectively. Obstructive hydrocephalus and acute infarct (elbow arrow) in pons (due to vasculitis) are also seen. Assigned score of 7 was consistent with tubercular meningitis.
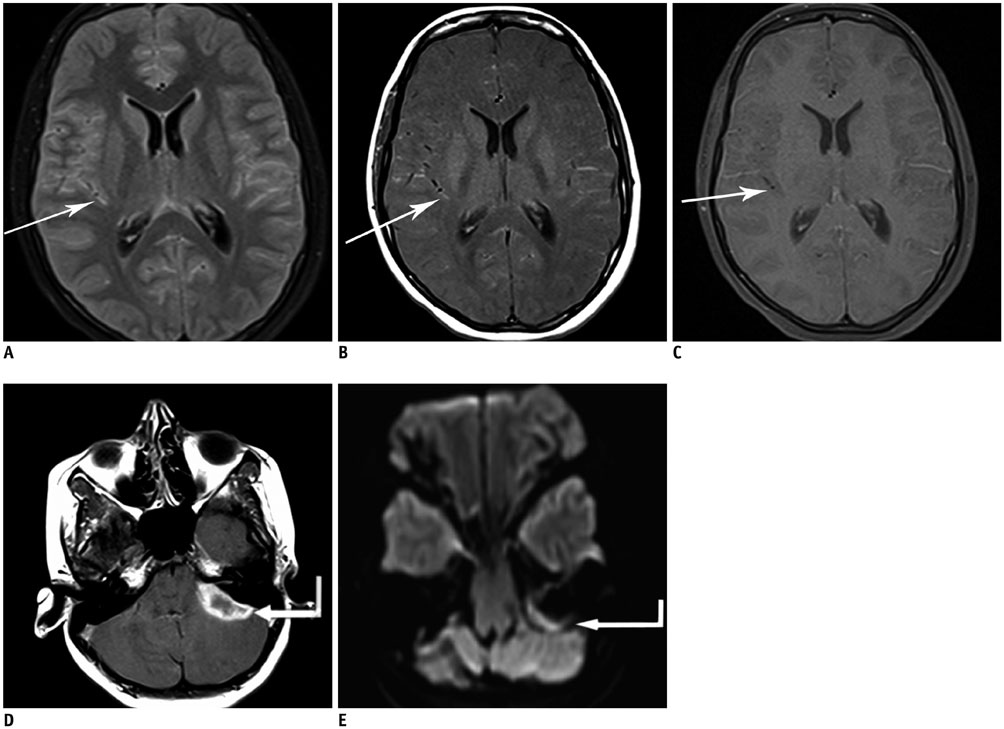
Fig. 3 MR imaging in 17-year-old female with pyogenic meningitis. CE-FLAIR (A), CE-T1W with MT (B, D) CE-T1W with FS (C), images DWI (E) reveal better enhancement on CE-FLAIR sequence (arrows), compared to grade 1 enhancement on CE-T1W sequences with MT and hardly any enhancement on CE-T1W sequence with FS. Assigned score of 4 was overlapping, but subdural empyema (elbow arrows) with diffusion restriction (seen along left cerebello-pontine angle) favored pyogenic etiology.
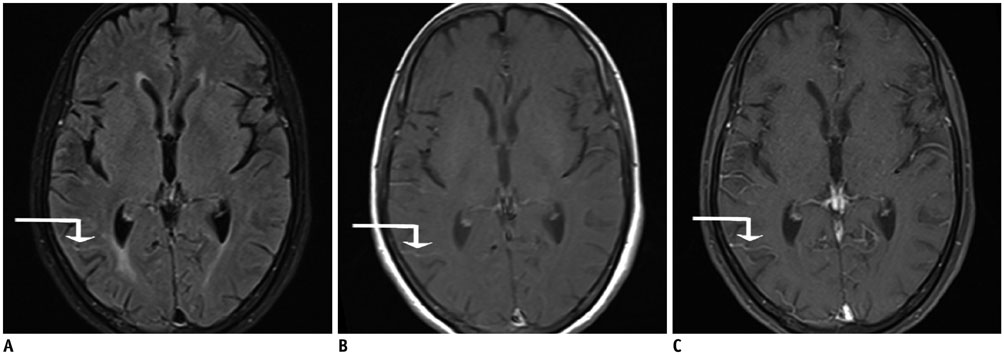
Fig. 4 MR imaging in 66-year-old female with viral meningitis. CE-FLAIR (A), CE-T1W with MT (B), CE-T1W with FS images (C) reveal grade 1 enhancement only on CE-FLAIR sequence (elbow arrows). No vascular enhancement is discernible. Assigned score of 1 in this case was consistent with viral etiology.
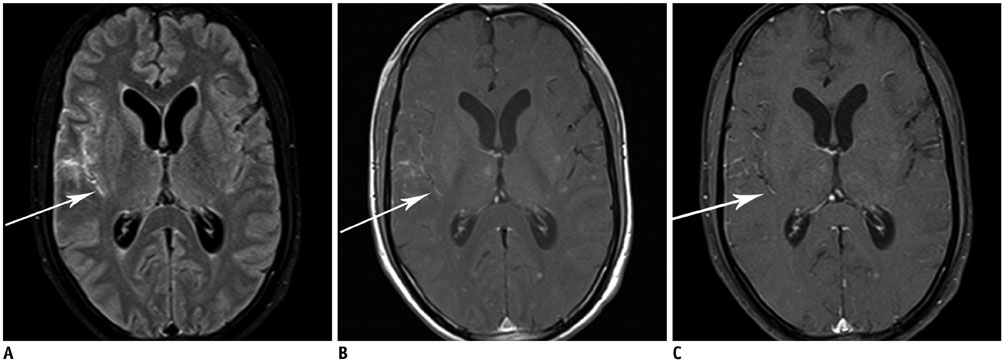
Fig. 5 MR imaging in 32-year-old male presenting with fever, headache and vomiting. CE-FLAIR (A), CE-T1W with MT (B), CE-T1W with FS images (C) reveal grade 2 enhancement on CE-FLAIR sequence, compared to grade 1 enhancement on CE-T1W sequences with MT and FS (arrows). This case was falsely interpreted as pyogenic instead of tubercular meningitis on basis of assigned score of 2.
Cited by 1 articles
-
Age of Data in Contemporary Research Articles Published in Representative General Radiology Journals
Ji Hun Kang, Dong Hwan Kim, Seong Ho Park, Jung Hwan Baek
Korean J Radiol. 2018;19(6):1172-1178. doi: 10.3348/kjr.2018.19.6.1172.
Reference
-
1. Ahmad A, Azad S, Azad R. Differentiation of leptomeningeal and vascular enhancement on post-contrast FLAIR MRI sequence: role in early detection of infectious meningitis. J Clin Diagn Res. 2015; 9:TC08–TC12.2. Finelli DA, Hurst GC, Gullapali RP, Bellon EM. Improved contrast of enhancing brain lesions on postgadolinium, T1-weighted spin-echo images with use of magnetization transfer. Radiology. 1994; 190:553–559.3. Kastrup O, Wanke I, Maschke M. Neuroimaging of infections. NeuroRx. 2005; 2:324–332.4. Kamra P, Azad R, Prasad KN, Jha S, Pradhan S, Gupta RK. Infectious meningitis: prospective evaluation with magnetization transfer MRI. Br J Radiol. 2004; 77:387–394.5. Galassi W, Phuttharak W, Hesselink JR, Healy JF, Dietrich RB, Imbesi SG. Intracranial meningeal disease: comparison of contrast-enhanced MR imaging with fluid-attenuated inversion recovery and fat-suppressed T1-weighted sequences. AJNR Am J Neuroradiol. 2005; 26:553–559.6. Singh SK, Leeds NE, Ginsberg LE. MR imaging of leptomeningeal metastases: comparison of three sequences. AJNR Am J Neuroradiol. 2002; 23:817–821.7. Mehta RC, Pike GB, Haros SP, Enzmann DR. Central nervous system tumor, infection, and infarction: detection with gadolinium-enhanced magnetization transfer MR imaging. Radiology. 1995; 195:41–46.8. Dousset V, Armand JP, Lacoste D, Mièze S, Letenneur L, Dartigues JF, et al. Magnetization transfer study of HIV encephalitis and progressive multifocal leukoencephalopathy. Groupe d’Epidémiologie Clinique du SIDA en Aquitaine. AJNR Am J Neuroradiol. 1997; 18:895–890.9. Burke JW, Mathews VP, Elster AD, Ulmer JL, McLean FM, Davis SB. Contrast-enhanced magnetization transfer saturation imaging improves MR detection of herpes simplex encephalitis. AJNR Am J Neuroradiol. 1996; 17:773–776.10. Kamran S, Bener AB, Alper D, Bakshi R. Role of fluidattenuated inversion recovery in the diagnosis of meningitis: comparison with contrast-enhanced magnetic resonance imaging. J Comput Assist Tomogr. 2004; 28:68–72.11. Mathews VP, Caldemeyer KS, Lowe MJ, Greenspan SL, Weber DM, Ulmer JL. Brain: gadolinium-enhanced fast fluidattenuated inversion-recovery MR imaging. Radiology. 1999; 211:257–263.12. Gupta RK, Kathuria MK, Pradhan S. Magnetization transfer MR imaging in CNS tuberculosis. AJNR Am J Neuroradiol. 1999; 20:867–875.13. Singer MB, Atlas SW, Drayer BP. Subarachnoid space disease: diagnosis with fluid-attenuated inversion-recovery MR imaging and comparison with gadolinium-enhanced spin-echo MR imaging--blinded reader study. Radiology. 1998; 208:417–422.14. Tsuchiya K, Inaoka S, Mizutani Y, Hachiya J. Fast fluid-attenuated inversion-recovery MR of intracranial infections. AJNR Am J Neuroradiol. 1997; 18:909–913.15. Vaswani AK, Nizamani WM, Ali M, Aneel G, Shahani BK, Hussain S. Diagnostic accuracy of contrast-enhanced FLAIR magnetic resonance imaging in diagnosis of meningitis correlated with CSF analysis. ISRN Radiol. 2014; 2014:578–586.16. De Coene B, Hajnal JV, Gatehouse P, Longmore DB, White SJ, Oatridge A, et al. MR of the brain using fluid-attenuated inversion recovery (FLAIR) pulse sequences. AJNR Am J Neuroradiol. 1992; 13:1555–1564.17. Parmar H, Sitoh YY, Anand P, Chua V, Hui F. Contrast-enhanced flair imaging in the evaluation of infectious leptomeningeal diseases. Eur J Radiol. 2006; 58:89–95.18. Melhem ER, Jara H, Eustace S. Fluid-attenuated inversion recovery MR imaging: identification of protein concentration thresholds for CSF hyperintensity. AJR Am J Roentgenol. 1997; 169:859–862.19. Taoka T, Yuh WT, White ML, Quets JP, Maley JE, Ueda T. Sulcal hyperintensity on fluid-attenuated inversion recovery mr images in patients without apparent cerebrospinal fluid abnormality. AJR Am J Roentgenol. 2001; 176:519–524.20. Mathews VP, Kuharik MA, Edwards MK, D’Amour PG, Azzarelli B, Dreesen RG. Dyke award. Gd-DTPA-enhanced MR imaging of experimental bacterial meningitis: evaluation and comparison with CT. AJR Am J Roentgenol. 1989; 152:131–136.21. Lee EK, Lee EJ, Kim S, Lee YS. Importance of contrastenhanced fluid-attenuated inversion recovery magnetic resonance imaging in various intracranial pathologic conditions. Korean J Radiol. 2016; 17:127–141.22. Capone PM, Scheller JM. Neuroimaging of infectious disease. Neurol Clin. 2014; 32:127–145.23. Splendiani A, Puglielli E, De Amicis R, Necozione S, Masciocchi C, Gallucci M. Contrast-enhanced FLAIR in the early diagnosis of infectious meningitis. Neuroradiology. 2005; 47:591–598.24. Quint DJ, Eldevik OP, Cohen JK. Magnetic resonance imaging of normal meningeal enhancement at 1.5 T. Acad Radiol. 1996; 3:463–468.25. Joosten AA, van der Valk PD, Geelen JA, Severin WP, Jansen Steur EN. Tuberculous meningitis: pitfalls in diagnosis. Acta Neurol Scand. 2000; 102:388–394.26. Grossman SA, Krabak MJ. Leptomeningeal carcinomatosis. Cancer Treat Rev. 1999; 25:103–119.27. Hughes DC, Raghavan A, Mordekar SR, Griffiths PD, Connolly DJ. Role of imaging in the diagnosis of acute bacterial meningitis and its complications. Postgrad Med J. 2010; 86:478–485.28. Upadhyayula S. Question 2 * is there a role for MRI as an adjunct for diagnosing bacterial meningitis? Arch Dis Child. 2013; 98:388–390.29. Lagi F, Bartalesi F, Pecile P, Biagioli T, Caldini AL, Fanelli A, et al. Proposal for a new score-based approach to improve efficiency of diagnostic laboratory workflow for acute bacterial meningitis in adults. J Clin Microbiol. 2016; 54:1851–1854.30. Schutte CM, van der Meyden CH. A prospective study of Glasgow Coma Scale (GCS), age, CSF-neutrophil count, and CSF-protein and glucose levels as prognostic indicators in 100 adult patients with meningitis. J Infect. 1998; 37:112–115.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- T1-, T2-weighted, and FLAIR Imaging: Clinical Application
- T1-weighted FLAIR MR Imaging for the Evaluation of Enhancing Brain Tumors: Comparison with Spin Echo Imaging
- T1-weighted MR Imaging of the Neonatal Brain at 3.0 Tesla: Comparison of Spin Echo, Fast Inversion Recovery, and Magnetization-prepared Three Dimensional Gradient Echo Techniques
- MR Imaging of Articular Cartilage: Comparison of Magnetization Transfer Contrast and Fat - Suppression inMultiplanar and 3D Gradient-Echo, Spin-Echo, Turbo Spin-Echo Techniques
- Importance of Contrast-Enhanced Fluid-Attenuated Inversion Recovery Magnetic Resonance Imaging in Various Intracranial Pathologic Conditions
