Imaging Features of Soft-Tissue Calcifications and Related Diseases: A Systematic Approach
- Affiliations
-
- 1Department of Radiology, Wan Fang Hospital, Taipei Medical University, Taipei 116, Taiwan. wingchan@tmu.edu.tw
- 2Department of Radiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei 110, Taiwan.
- 3Department of Radiology, Dongguk University Gyeongju Hospital, Gyeongju 38067, Korea.
- 4Department of Radiology, University of California, Davis, CA 95817, USA.
- 5Department of Radiology, Beth Israel Deaconess Medical Center, Boston, MA 02215, USA.
- KMID: 2424854
- DOI: http://doi.org/10.3348/kjr.2018.19.6.1147
Abstract
- Soft-tissue calcification refers to a broad category of lesions. Calcifications are frequently identified by radiologists in daily practice. Using a simple algorithm based on the distribution pattern of the lesions and detailed clinical information, these calcified lesions can be systematically evaluated. The distribution pattern of the calcific deposits enables initial division into calcinosis circumscripta and calcinosis universalis. Using laboratory test results (serum calcium and phosphate levels) and clinical history, calcinosis circumscripta can be further categorized into four subtypes: dystrophic, iatrogenic, metastatic, and idiopathic calcification. This pictorial essay presents a systematic approach to the imaging features of soft-tissue calcifications and related diseases.
Keyword
MeSH Terms
Figure
-
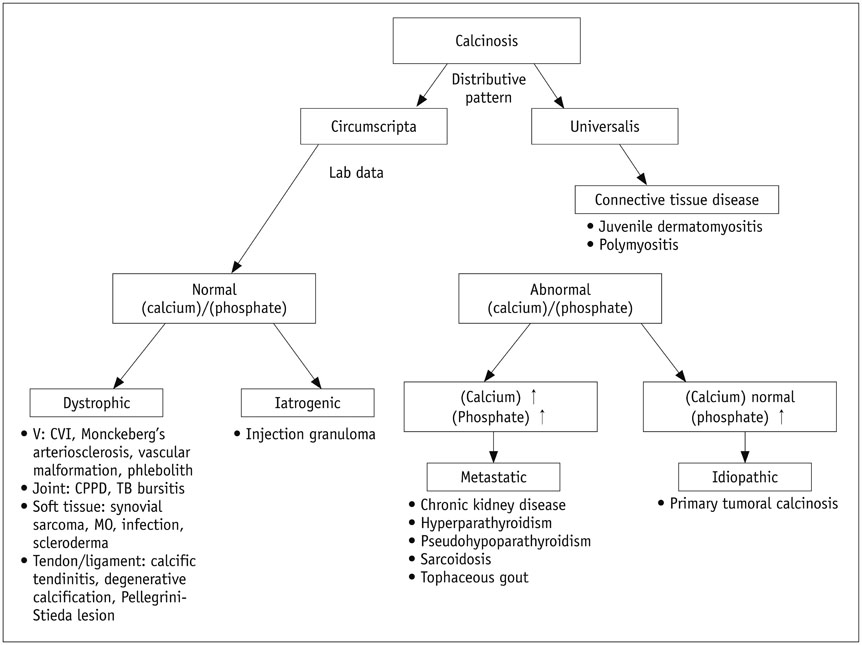
Fig. 1 Evaluation flowchart enabling division of calcified lesions into calcinosis circumscripta and calcinosis universalis based on distribution patterns. Using laboratory testing, calcinosis circumscripta can be categorized into dystrophic, iatrogenic, metastatic, and idiopathic calcification subtypes. CPPD = calcium pyrophosphate dihydrate crystal deposition, CVI = chronic venous insufficiency, MO = myositis ossificans, TB bursitis = tuberculous bursitis, V= vascular

Fig. 2 Calcinosis universalis in 56-year-old man with dermatomyositis who presented with longstanding skin and muscle pain. Coronal computed tomography image reveals calcinosis universalis, in which extensive calcification (arrowheads) is distributed in sheet-like pattern in bilateral gluteal regions and lower extremities.

Fig. 3 CVI in 93-year-old woman with ulcer on her left leg. Anteroposterior radiograph of knee reveals characteristic trabecular calcification (arrow) at medial aspect of left tibia resulting from CVI. CVI = chronic venous insufficiency
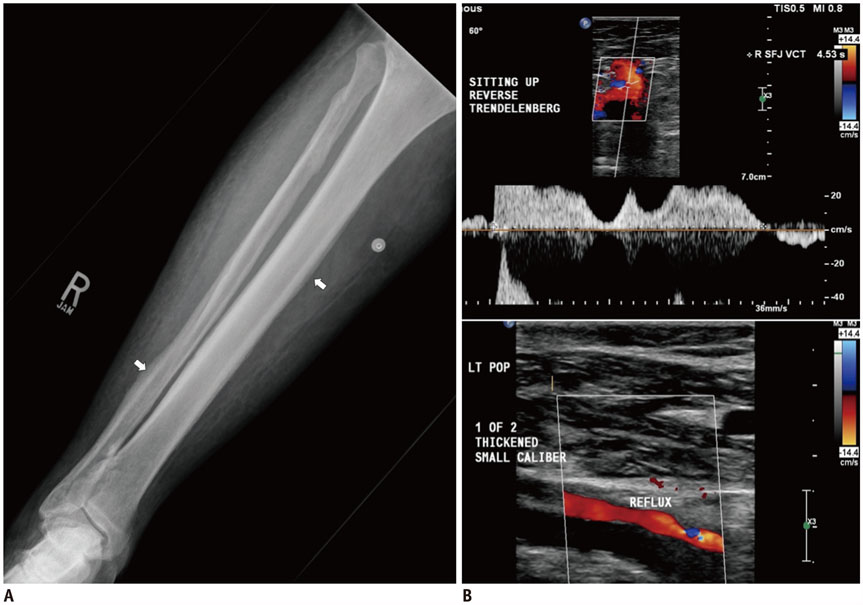
Fig. 4 CVI in 77-year-old woman with history of lower extremity deep venous thrombosis, who presented with pain and swelling bilaterally in lower legs. A. Anteroposterior radiograph of right lower leg revealing wavy and continuous periosteal reaction (arrows) in tibia and fibula. B. Color Doppler ultrasound revealing superficial venous reflux at right saphenofemoral junction (reflux time, 4.5 seconds after reverse Trendelenburg) and deep venous reflux at left popliteal vein.

Fig. 5 Mönckeberg's arteriosclerosis in 70-year-old man with recent history of falling and knee pain. Lateral radiograph of knee revealing extensive calcification of femoral and popliteal arteries that appears with “railroad track” pattern (arrowheads), indicating Mönckeberg's arteriosclerosis.

Fig. 6 57-year-old woman with phleboliths who presented with mass along lateral aspect of her right ankle. Radiograph of right ankle joint revealing soft tissue swelling with round nodular opacity within (arrowheads), showing phleboliths.
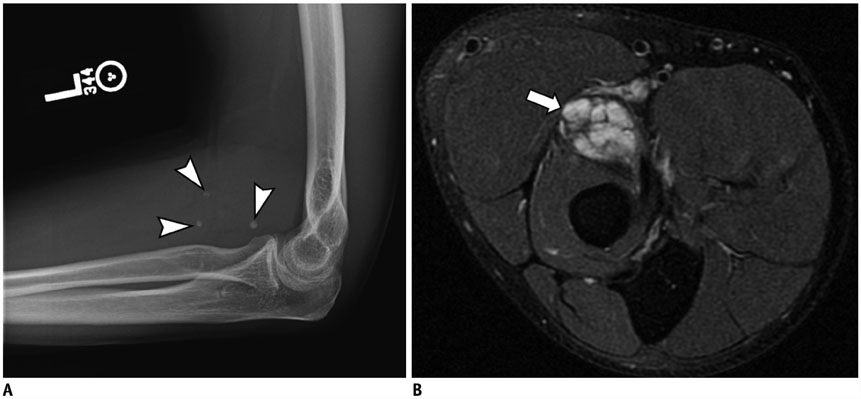
Fig. 7 38-year-old man with venous malformation who presented with fullness and mild pain in his left elbow. A. Lateral radiograph revealing presence of phleboliths (arrowheads). B. Axial T2-weighted fat-saturated MR images demonstrating hyperintensity in tubular structures (arrow), which are discrete vessels, indicating venous malformation. MR = magnetic resonance

Fig. 8 Venous malformation in 17-year-old girl. She presented with hard mass in her lower right leg and 1-year history of walking pain. No trauma history was reported. Lateral radiograph revealing calcification (arrowheads) at posterior aspect of lower right extremity. Further MR imaging confirmed venous malformation (not shown).
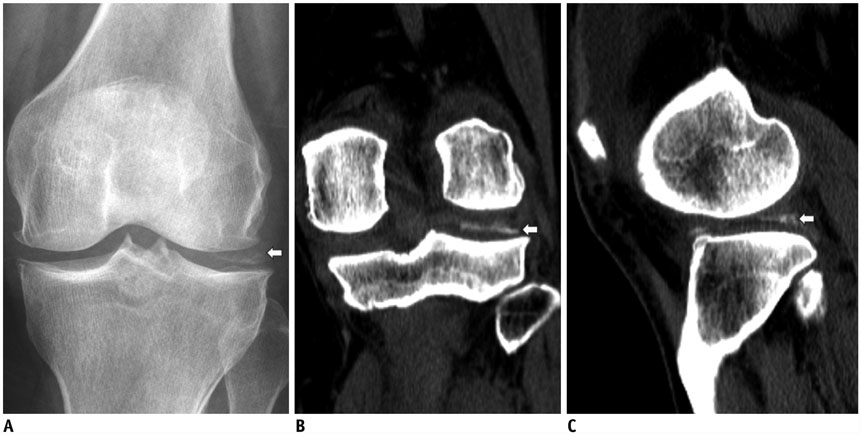
Fig. 9 Calcium pyrophosphate dihydrate crystal doposition disease in 56-year-old woman who experienced chronic left knee pain and swelling for 1 day after minor fall. A. Anteroposterior radiograph of knee revealing calcification at lateral aspect of tibiofemoral joint (arrow). B. Coronal computed tomography view revealing chondrocalcinosis at lateral meniscus (arrow). C. Sagittal computed tomography view revealing chondrocalcinosis situated at posterior horn of lateral meniscus (arrow).

Fig. 10 TB trochanteric bursitis in 70-year-old man with left hip pain for 3 years. A. Anteroposterior radiograph of left hip joint revealing bony destruction of greater trochanter and ossification in subgluteus medius bursa region (arrow). B. Coronal T1-weighted fat-suppressed post contrast images reveals marked enhancement of enlarged bursae with irregular, nodular-like synovia (arrowheads).

Fig. 11 Synovial sarcoma in 54-year-old man with palpable mass in his right foot. A. Anteroposterior radiograph of foot revealing calcified soft-tissue mass (arrow) between second and third proximal phalanges with extrinsic bone erosions. B. Axial T1-weighted fat-suppressed post-contrast images demonstrating heterogeneous enhancement of mass lesion (arrowheads), which dorsally extended between second and third proximal phalanges. Low signal intensity changes within lesion indicate calcification.

Fig. 12 Mature MO in 28-year-old man with 3-month history of hamstring injury, who presented with right groin pain. A. Anteroposterior radiograph of pelvis revealing well-circumscribed ossified mass (arrow) located proximally in soft tissue of right thigh. B. Axial computed tomography view revealing distinct margin of lesion with peripheral mature ossification (arrow) within right adductor magnus muscle.

Fig. 13 51-year-old South American woman with cysticercosis infection who presented with right knee pain. Anteroposterior radiograph of right knee revealing typical rice-grain calcification (arrows) in distal muscles of right femur and calf, characteristic of cysticercosis infection.

Fig. 14 Scleroderma in 71-year-old woman presenting with left hand pain. Anteroposterior radiograph of left hand revealing multiple dense and well-defined calcified nodules (arrowheads) in soft tissues of first to fourth phalanges, confirming her medical history of scleroderma.

Fig. 15 70-year-old man with degenerative calcification of Achilles tendon, who injured his Achilles tendon 20 years previously. Lateral radiograph of left ankle joint revealing partial ossification (arrowheads) of Achilles tendon, type 2, confirming degenerative calcification.

Fig. 16 Calcific tendinitis in 45-year-old woman with left shoulder pain. Anteroposterior radiograph of left shoulder joint revealing calcification (arrow) with ill-defined margin located at insertion of supraspinatus tendon, suggestive of resorptive phase of calcific tendinitis.
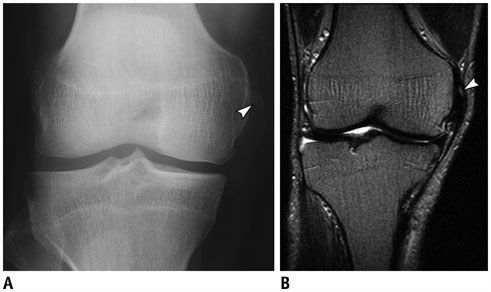
Fig. 17 Pellegrini-Stieda syndrome in 60-year-old woman with right knee pain. A. Anteroposterior radiograph of right knee of revealing linear calcification (arrowhead) abutting medial femoral condyle. B. Coronal T2-weighted MR images confirming lesion is situated in region of proximal attachment of medial collateral ligament (arrowhead).

Fig. 18 Injection granulomas in 69-year-old woman. Radiograph revealing multiple foci of calcifications (arrows) superimposed bilaterally over buttocks.

Fig. 19 Uremic tumoral calcinosis in 56-year-old woman who presented with palpable mass at right elbow. Anteroposterior radiograph of elbow joint revealing multilobulated, rounded, calcified lesions (arrowhead) in soft tissues located at medial aspect of her elbow, indicating uremic tumoral calcinosis.
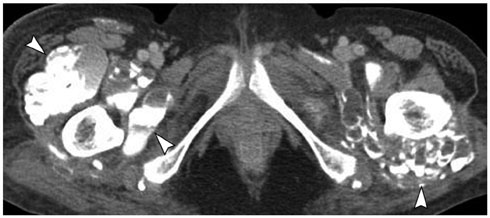
Fig. 20 Uremic tumoral calcinosis in 55-year-old woman with bilateral palpable painless masses in buttocks. Axial computed tomography scan reveals multilobulated calcified cystic lesions with sedimentation (arrowheads) at greater trochanteric bursa (bilaterally), which are indistinguishable from primary tumoral calcinosis.

Fig. 21 Uremic tumoral calcinosis in 43-year-old woman with chronic renal failure who had undergone hemodialysis for 6 years and presented with 2-month history of palpable mass in her right gluteal region. A. Anteroposterior radiograph of pelvis revealing massive periarticular calcinosis (arrowheads) abutting right hip joint, which is indistinguishable from primary tumoral calcinosis. B. Coronal T2-weighted MR image revealing heterogeneous intensity of calcinosis (arrowheads).
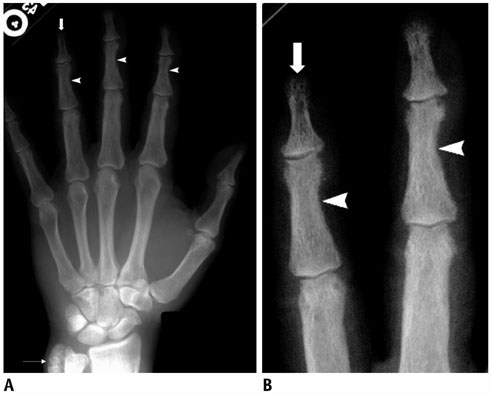
Fig. 22 Hyperparathyroidism in 47-year-old woman who presented with hand pain. A. Anteroposterior radiograph of right hand reveals subperiosteal bone resorption along radial aspects of middle phalanges of second, third, and fourth fingers (arrowheads). Thin-arrow identifies lobulated calcified mass abutting right ulna. B. Magnification view reveals bone erosion of distal phalangeal tufts, resulting in acro-osteolysis (arrow). Arrowheads shows subperiosteal bone resorption.

Fig. 23 Pseudohypoparathyroidism in 22-year-old woman with short stature and intellectual disability. Anteroposterior radiograph of left hand revealing shortened first, fourth, and fifth metacarpal bones (arrowheads) with calcification adjacent to fourth metacarpal bone.
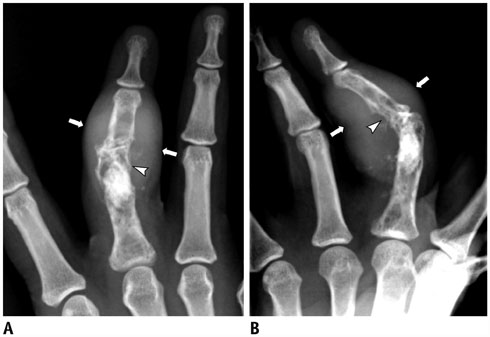
Fig. 24 Type 3 sarcoid dactylitis in 51-year-old woman with right hand pain. Anteroposterior (A), and lateral (B) radiograph of right hand demonstrating radiolucent lesions with “lace-like” patterns at proximal and middle phalanx of third digit (arrowheads), and fusiform thickening of infiltrated soft tissue (arrows) resulting from sarcoid dactylitis.

Fig. 25 Gout in 82-year-old man with right foot pain. Anteroposterior radiograph of right foot demonstrating radiopaque lesion (gouty tophus) with juxta-articular erosion and soft tissue swelling at first metatarsophalangeal joint (arrow). Note that joint space and bone density are normal, with absence of intra-articular erosions.
Reference
-
1. Santili C, Akkari M, Waisberg G, Kessler C, Alcantara Td, Delai PL. Calcinosis universalis: a rare diagnosis. J Pediatr Orthop B. 2005; 14:294–298.
Article2. Abdallah-Lotf M, Grasland A, Vinceneux P, Sigal-Grinberg M. Regression of cutis calcinosis with diltiazem in adult dermatomyositis. Eur J Dermatol. 2005; 15:102–104.3. Olsen KM, Chew FS. Tumoral calcinosis: pearls, polemics, and alternative possibilities. Radiographics. 2006; 26:871–885.
Article4. Chander S, Gordon P. Soft tissue and subcutaneous calcification in connective tissue diseases. Curr Opin Rheumatol. 2012; 24:158–164.
Article5. Stewart VL, Herling P, Dalinka MK. Calcification in soft tissues. JAMA. 1983; 250:78–81.
Article6. Lafferty FW, Reynolds ES, Pearson OH. Tumoral calcinosis: a metabolic disease of obscure etiology. Am J Med. 1965; 38:105–118.7. Tokoro S, Satoh T, Okubo Y, Igawa K, Yokozeki H. Latent dystrophic subcutaneous calcification in patients with chronic venous insufficiency. Acta Derm Venereol. 2009; 89:505–508.
Article8. Rana RS, Wu JS, Eisenberg RL. Periosteal reaction. AJR Am J Roentgenol. 2009; 193:W259–W272.
Article9. Kim H, Greenberg JS, Javitt MC. Breast calcifications due to Mönckeberg medial calcific sclerosis. Radiographics. 1999; 19:1401–1403.10. Tahmasbi-Arashlow M, Barghan S, Kashtwari D, Nair MK. Radiographic manifestations of Mönckeberg arteriosclerosis in the head and neck region. Imaging Sci Dent. 2016; 46:53–56.
Article11. Flors L, Leiva-Salinas C, Maged IM, Norton PT, Matsumoto AH, Angle JF, et al. MR imaging of soft-tissue vascular malformations: diagnosis, classification, and therapy follow-up. Radiographics. 2011; 31:1321–1340. discussion 1340-1341.
Article12. Fayad LM, Hazirolan T, Bluemke D, Mitchell S. Vascular malformations in the extremities: emphasis on MR imaging features that guide treatment options. Skeletal Radiol. 2006; 35:127–137.
Article13. Ernemann U, Kramer U, Miller S, Bisdas S, Rebmann H, Breuninger H, et al. Current concepts in the classification, diagnosis and treatment of vascular anomalies. Eur J Radiol. 2010; 75:2–11.
Article14. Steinbach LS, Resnick D. Calcium pyrophosphate dihydrate crystal deposition disease revisited. Radiology. 1996; 200:1–9.
Article15. Ogata M. [A clinical study of calcium pyrophosphate dihydrate crystal deposition disease]. Nihon Seikeigeka Gakkai Zasshi. 1985; 59:819–834.16. Jacobson JA, Girish G, Jiang Y, Sabb BJ. Radiographic evaluation of arthritis: degenerative joint disease and variations. Radiology. 2008; 248:737–747.
Article17. Westall J. Tuberculosis levelling off worldwide. BMJ. 1997; 314:921.
Article18. De Backer AI, Vanhoenacker FM, Sanghvi DA. Imaging features of extraaxial musculoskeletal tuberculosis. Indian J Radiol Imaging. 2009; 19:176–186.
Article19. Hugosson C, Nyman RS, Brismar J, Larsson SG, Lindahl S, Lundstedt C. Imaging of tuberculosis. V. Peripheral osteoarticular and soft-tissue tuberculosis. Acta Radiol. 1996; 37:512–516.20. Jaovisidha S, Chen C, Ryu KN, Siriwongpairat P, Pekanan P, Sartoris DJ, et al. Tuberculous tenosynovitis and bursitis: imaging findings in 21 cases. Radiology. 1996; 201:507–513.
Article21. Meyerding HW, Mroz RJ. Tuberculosis of the greater trochanter. JAMA. 1933; 101:1308–1313.
Article22. Rehm-Graves S, Weinstein AJ, Calabrese LH, Cook SA, Boumphrey FR. Tuberculosis of the greater trochanteric bursa. Arthritis Rheum. 1983; 26:77–81.
Article23. Murphey MD, Gibson MS, Jennings BT, Crespo-Rodríguez AM, Fanburg-Smith J, Gajewski DA. From the archives of the AFIP: imaging of synovial sarcoma with radiologic-pathologic correlation. Radiographics. 2006; 26:1543–1565.24. Jones BC, Sundaram M, Kransdorf MJ. Synovial sarcoma: MR imaging findings in 34 patients. AJR Am J Roentgenol. 1993; 161:827–830.
Article25. Kransdorf MJ, Meis JM. From the archives of the AFIP. Extraskeletal osseous and cartilaginous tumors of the extremities. Radiographics. 1993; 13:853–884.
Article26. Nuovo MA, Norman A, Chumas J, Ackerman LV. Myositis ossificans with atypical clinical, radiographic, or pathologic findings: a review of 23 cases. Skeletal Radiol. 1992; 21:87–101.
Article27. Bhalla A, Sood A, Sachdev A, Varma V. Disseminated cysticercosis: a case report and review of the literature. J Med Case Rep. 2008; 2:137.
Article28. Roche CJ, O'Keeffe DP, Lee WK, Duddalwar VA, Torreggiani WC, Curtis JM. Selections from the buffet of food signs in radiology. Radiographics. 2002; 22:1369–1384.
Article29. Naik D, Srinath M, Kumar A. Soft tissue cysticercosis - Ultrasonographic spectrum of the disease. Indian J Radiol Imaging. 2011; 21:60–62.
Article30. Narváez JA, Narváez J, Ortega R, Aguilera C, Sánchez A, Andía E. Painful heel: MR imaging findings. Radiographics. 2000; 20:333–352.
Article31. Richards PJ, Braid JC, Carmont MR, Maffulli N. Achilles tendon ossification: pathology, imaging and aetiology. Disabil Rehabil. 2008; 30:1651–1665.
Article32. Morris KL, Giacopelli JA, Granoff D. Classifications of radiopaque lesions of the tendo Achillis. J Foot Surg. 1990; 29:533–542.33. Speed CA, Hazleman BL. Calcific tendinitis of the shoulder. N Engl J Med. 1999; 340:1582–1584.
Article34. Serafini G, Sconfienza LM, Lacelli F, Silvestri E, Aliprandi A, Sardanelli F. Rotator cuff calcific tendonitis: short-term and 10-year outcomes after two-needle us-guided percutaneous treatment--nonrandomized controlled trial. Radiology. 2009; 252:157–164.35. ViGario GD, Keats TE. Localization of calcific deposits in the shoulder. Am J Roentgenol Radium Ther Nucl Med. 1970; 108:806–811.
Article36. Mendes LF, Pretterklieber ML, Cho JH, Garcia GM, Resnick DL, Chung CB. Pellegrini-Stieda disease: a heterogeneous disorder not synonymous with ossification/calcification of the tibial collateral ligament-anatomic and imaging investigation. Skeletal Radiol. 2006; 35:916–922.
Article37. Cockshott WP, Thompson GT, Howlett LJ, Seeley ET. Intramuscular or intralipomatous injections? N Engl J Med. 1982; 307:356–358.
Article38. Prosch H, Mirzaei S, Oschatz E, Strasser G, Huber M, Mostbeck G. Case report: gluteal injection site granulomas: false positive finding on FDG-PET in patients with non-small cell lung cancer. Br J Radiol. 2005; 78:758–761.39. Stein L, Elsayes KM, Wagner-Bartak N. Subcutaneous abdominal wall masses: radiological reasoning. AJR Am J Roentgenol. 2012; 198:W146–W151.
Article40. Degrassi F, Quaia E, Martingano P, Cavallaro M, Cova MA. Imaging of haemodialysis: renal and extrarenal findings. Insights Imaging. 2015; 6:309–321.
Article41. Gordon LF, Arger PH, Dalinka MK, Coleman BG. Computed tomography in soft tissue calcification layering. J Comput Assist Tomogr. 1984; 8:71–73.
Article42. Chang CY, Rosenthal DI, Mitchell DM, Handa A, Kattapuram SV, Huang AJ. Imaging findings of metabolic bone disease. Radiographics. 2016; 36:1871–1887.
Article43. Khan AA, Hanley DA, Rizzoli R, Bollerslev J, Young JE, Rejnmark L, et al. Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos Int. 2017; 28:1–19.
Article44. Khan A, Bilezikian J. Primary hyperparathyroidism: pathophysiology and impact on bone. CMAJ. 2000; 163:184–187.45. Wilson LC, Hall CM. Albright's hereditary osteodystrophy and pseudohypoparathyroidism. Semin Musculoskelet Radiol. 2002; 6:273–283.
Article46. Mantovani G. Clinical review: pseudohypoparathyroidism: diagnosis and treatment. J Clin Endocrinol Metab. 2011; 96:3020–3030.47. Moore SL, Teirstein AE. Musculoskeletal sarcoidosis: spectrum of appearances at MR imaging. Radiographics. 2003; 23:1389–1399.
Article48. James DG, Neville E, Carstairs LS. Bone and joint sarcoidosis. Semin Arthritis Rheum. 1976; 6:53–81.
Article49. Aptel S, Lecocq-Teixeira S, Olivier P, Regent D, Teixeira PG, Blum A. Multimodality evaluation of musculoskeletal sarcoidosis: imaging findings and literature review. Diagn Interv Imaging. 2016; 97:5–18.
Article50. Koyama T, Ueda H, Togashi K, Umeoka S, Kataoka M, Nagai S. Radiologic manifestations of sarcoidosis in various organs. Radiographics. 2004; 24:87–104.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiological Features of Soft Tissue Calcification: A Pictorial Essay
- Sonographic Features of Common Soft Tissue Masses in the Extremities
- Soft Tissue Disease around the Hip
- CT and MRI Features of Localized Peritumoral Amyloidosis in a Patient with Head and Neck MucosaAssociated Lymphoid Tissue Lymphoma: A Case Report
- Diagnostic Approach to a Soft Tissue Mass
