J Dent Anesth Pain Med.
2018 Aug;18(4):261-265. 10.17245/jdapm.2018.18.4.261.
Use of sugammadex in Rett syndrome: A case report
- Affiliations
-
- 1Department of Anesthesiology and Reanimation, Erzincan Binali Yıldırım University, Faculty Of Medicine, Erzincan, Turkey. ilkeser2004@gmail.com
- KMID: 2419068
- DOI: http://doi.org/10.17245/jdapm.2018.18.4.261
Abstract
- Rett syndrome (RS) is a neurodevelopmental disorder characterized by loss of cognitive, motor, and social skills, epilepsy, autistic behavior, abnormal airway patterns, gastroesophageal reflux, nutritional problems, and severe scoliosis. Although girls with RS show normal or near-normal growth until 6-8 months, they lose their skills after that. The anesthetic management of these patients requires care because of all these clinical features. Especially in the postoperative period, prolonged apnea is common and extubation is delayed. In this case report, the effect of using sugammadex was presented in a 16-year-old girl with RS. The patient's all bimaxillary teeth and 4 wisdom teeth were extracted under general anesthesia in one session with minimal surgical trauma and moderate bleeding. Sugammadex can be a rapid and reliable agent for the reversal of the neuromuscular block in neurodegenerative patients.
Keyword
MeSH Terms
Figure
-

Fig. 1 The patient's hands and legs
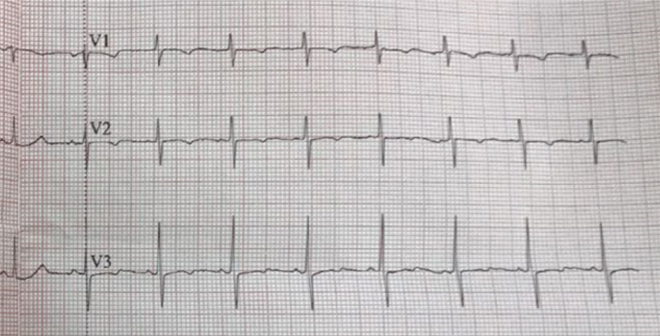
Fig. 2 Electrocardiograph
Reference
-
1. Berridge CW, Waterhouse BD. The locus coeruleusnoradrenergic system: modulation of behavioral state and state-dependent cognitive processes. Brain Res Rev. 2003; 42:33–84.
Article2. Karaca O, Pinar HU, Ekmekcioglu SE, Dogan R. Rett syndrome and anaesthetic management: a case report. Med Science. 2017; 6:122–124.
Article3. Kako H, Martin DP, Cartabuke R, Beebe A, Klamar J, Tobias JD. Perioperative management of a patient with Rett syndrome. Int J Clin Exp Med. 2013; 6:393–403.4. Huppke P, Laccone F, Kramer N, Engel W, Hanefeld F. Rett Syndrome: Analysis of MECPP2 and clinical characterization of 31 patients. Hum Mol Genet. 2000; 9:1369–1375.
Article5. Nho JS, Shin DS, Moon JY, Yi JW, Kang JM, Lee BJ, et al. Anesthetic management of an adult patient with Rett syndrome and limited mouth opening - a case report. Korean J Anesthesiol. 2011; 61:428–430.
Article6. Tofil NM, Buckmaster MA, Winkler MK, Callans BH, Islam MP, Percy AK. Deep sedation with propofol in patients with Rett syndrome. J Child Neurol. 2006; 21:210–213.
Article7. Gibert S, Sabourdin N, Louvet N, Moutard ML, Piat V, Guye ML, et al. Epileptogenic effect of sevoflurane: determination of the minimal alveolar concentration of sevoflurane associated with major epileptoid signs in children. Anesthesiology. 2012; 117:1253–1261.8. Cafiero T, DiMinno RM, DiIorio C. QT interval and QT dispersion during the induction of anesthesia and tracheal intubation: a comparison of remifentanil and fentanyl. Minerva Anestesiol. 2011; 77:160–165.9. Saarnivaara L, Simola M. Effects of four anticholinesterase-anticholinergic combination and tracheal extubation on QTc interval of the ECG, heart rate and arterial pressure. Acta Anaesth Scand. 1998; 42:460–463.
Article10. Kawasaki E, Mishima Y, Ito T, Ito A, Takaseya H, Kameyama N, et al. Anesthetic management of a patient with Rett syndrome associated with trismus and apnea attacks. Masui. 2012; 61:96–99.
