Trough level of infliximab is useful for assessing mucosal healing in Crohn's disease: a prospective cohort study
- Affiliations
-
- 1Department of Gastroenterology, Fukuoka University Chikushi Hospital, Chikushino, Japan. matsui@fukuoka-u.ac.jp
- 2Department of Medicine, Shiga University of Medical Science, Otsu, Japan.
- KMID: 2417674
- DOI: http://doi.org/10.5217/ir.2018.16.2.223
Abstract
- BACKGROUND/AIMS
Decreased trough levels of infliximab (TLI) and antibodies to infliximab (ATI) are associated with loss of response (LOR) in Crohn's disease. Two prospective studies were conducted to determine whether TLI or ATI better correlates with LOR (Study 1), and whether TLI could become a predictor of mucosal healing (MH) (Study 2).
METHODS
Study 1 was conducted in 108 patients, including those with LOR and remission to compare ATI and TLI in discriminating the 2 conditions based on receiver operating characteristic (ROC) curve analyses. Study 2 involved 35 patients who were evaluated endoscopically.
RESULTS
In Study 1, there were no differences between the 2 assays in ROC curve analyses; the TLI cutoff value for LOR was 2.6 µg/mL (sensitivity, 70.9%; specificity, 79.2%), and the ATI cutoff value was 4.9 µg/mL (sensitivity, 65.5%; specificity, 67.9%). The AUROC (area under the ROC curve) of TLI was greater than that of ATI. AUROC was useful for discriminating between the 2 conditions. In Study 2, the TLI was significantly higher in the colonic MH group than in the non-MH group (2.7 µg/mL vs. 0.5 µg/mL, P=0.032).
CONCLUSIONS
TLI is better than ATI for clinically diagnosing LOR, and a correlation was observed between TLI and colonic MH.
Keyword
MeSH Terms
Figure
-
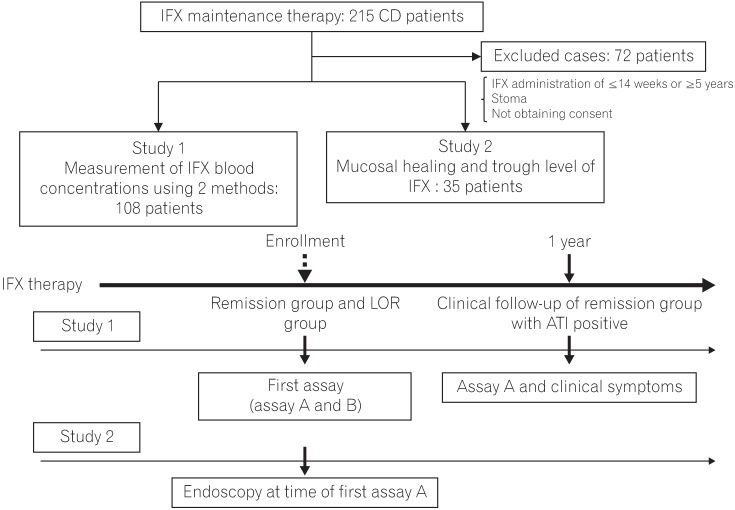
Fig. 1 Overview of study protocol, subject selection and inclusion criteria in Study. The inclusion criteria in Study 1 and Study 2 were: (1) efficacy of initial infusion of infliximab (IFX) was response, were undergoing maintenance therapy; (2) provided informed consent to blood sampling to measure IFX blood concentrations and to endoscopy; (3) their course could be followed up sufficiently; (4) their CDAI could be measured; and (5) were able to undergo colonoscopy or double-balloon enteroscopy within 2 months before or after the date of IFX blood concentration measurement. Exclusion criteria were: (1) continuous administration of IFX for ≤14 weeks or ≥5 years; (2) a stoma; or (3) not obtaining consent. A total of 72 patients were excluded. In the study design in Study 1, the first assay (assay A and B) was performed with patients divided into loss of response (LOR) group and remission group. Assay A and clinical symptoms in the antibodies to IFX (ATI)-positive patents in the remission group were checked after 1 year. In Study 2, endoscopic examination and assay A were performed after enrollment.
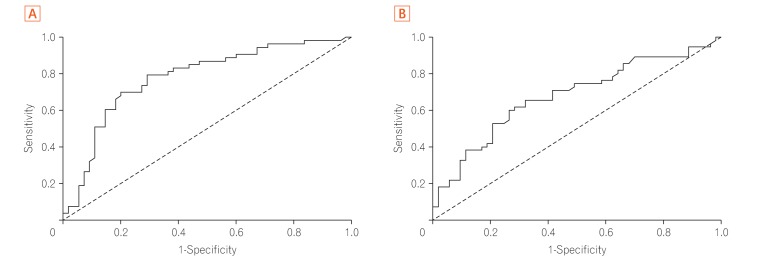
Fig. 2 Receiver operating characteristic (ROC) curve and cutoff value of infliximab (IFX) trough level and antibodies to IFX (ATI) by assay B (Study 1). (A) ROC curve-cutoff value of the IFX trough level in CD was calculated, as was association between IFX trough level and loss of response, with corresponding sensitivity and specificity for CD. Cutoff value, 2.6 µg/mL; area under the ROC curve (AUROC), 77.8. (B) ROC curve-cutoff value of ATI in CD was calculated, as was association between ATI and loss of response, with corresponding sensitivity and specificity for CD. Cutoff value, 4.9 µg/mL; AUROC, 67.9.
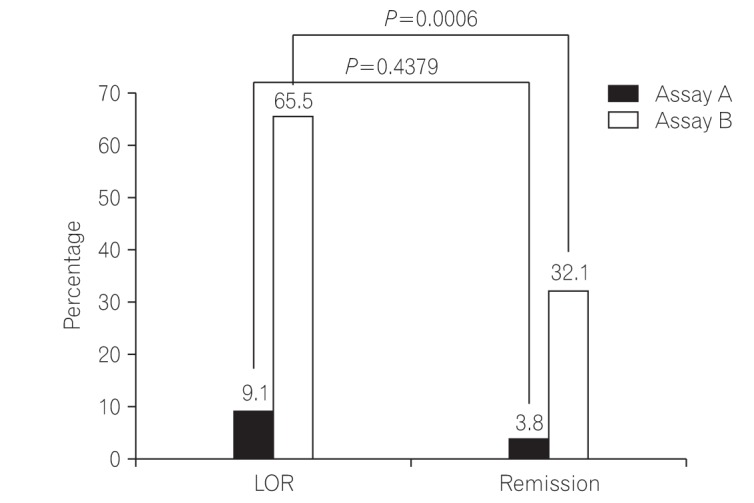
Fig. 3 Antibodies to infliximab (ATI)-positive rates in loss of response (LOR) group and in remission group. “ATI positive” was defined as ATI positivity in assay A and ATI of ≥4.9 µg/mL in assay B. Assay B was used to measure the percentage of patients with ATI in both the LOR and remission groups. ATI-positive rates with assays A and B, respectively, are 9.1% vs. 65.5% in the LOR group, and 3.8% vs. 32.1% in the remission group. Comparison of ATI-positive rates in the LOR and remission groups shows P=0.4379 with assay A, compared to P=0.0006 with assay B.
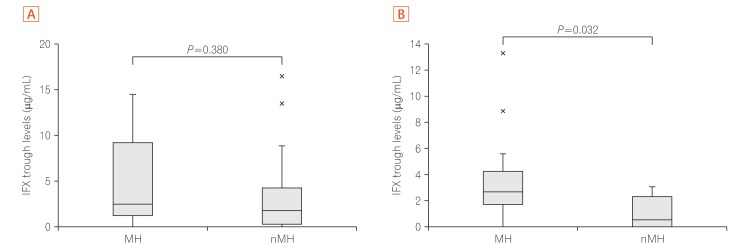
Fig. 4 A) Comparison of infliximab (IFX) trough levels between mucosal healing (MH) group and non-MH (nMH) group with lesions of small intestine (Study 2). MH occurred in 10 patients, and there were 21 patients in the nMH group. TLI (trough levels of infliximab; median values) in the MH and nMH groups were 2.5 µg/mL vs. 1.8 µg/mL, respectively. TLI in the MH and nMH groups showed no significant difference (P=0.380). Number of patients positive for antibodies to IFX (ATI) with assay A: 1 patient (10.0%) in the MH group and 3 patients (14.3%) in the nMH group. (B) Comparison of IFX trough levels between MH group and nMH group with lesions of large intestine (Study 2). There were 13 patients with MH and 8 patients in the nMH group. TLI (median values) in the MH and nMH groups were 2.7 µg/mL vs. 0.5 µg/mL, respectively. Comparison of TLI between the 2 groups showed a significant difference (P=0.032). Number of patients positive for ATI with Assay A: 0 patients (0.0%) in the MH group and 2 patients (25.0%) in the nMH group.
Cited by 1 articles
-
Potential Utility of Therapeutic Drug Monitoring of Adalimumab in Predicting Short-Term Mucosal Healing and Histologic Remission in Pediatric Crohn's Disease Patients
So Yoon Choi, Young Ok Choi, Yon Ho Choe, Ben Kang
J Korean Med Sci. 2020;35(16):e114. doi: 10.3346/jkms.2020.35.e114.
Reference
-
1. Gisbert JP, Panés J. Loss of response and requirement of infliximab dose intensification in Crohn's disease: a review. Am J Gastroenterol. 2009; 104:760–767. PMID: 19174781.
Article2. Ben-Horin S, Chowers Y. Review article: loss of response to anti-TNF treatments in Crohn's disease. Aliment Pharmacol Ther. 2011; 33:987–995. PMID: 21366636.
Article3. Danese S, Fiorino G, Reinisch W. Review article: causative factors and the clinical management of patients with Crohn’s disease who lose response to anti-TNF-alpha therapy. Aliment Pharmacol Ther. 2011; 34:1–10. PMID: 21539588.
Article4. Steenholdt C, Bendtzen K, Brynskov J, Thomsen OØ, Ainsworth MA. Cut-off levels and diagnostic accuracy of infliximab trough levels and anti-infliximab antibodies in Crohn's disease. Scand J Gastroenterol. 2011; 46:310–318. PMID: 21087119.
Article5. Vande Casteele N, Khanna R, Levesque BG, et al. The relationship between infliximab concentrations, antibodies to infliximab and disease activity in Crohn’s disease. Gut. 2015; 64:1539–1545. PMID: 25336114.
Article6. Maini RN, Breedveld FC, Kalden JR, et al. Therapeutic efficacy of multiple intravenous infusions of anti-tumor necrosis factor alpha monoclonal antibody combined with low-dose weekly methotrexate in rheumatoid arthritis. Arthritis Rheum. 1998; 41:1552–1563. PMID: 9751087.
Article7. Imaeda H, Takahashi K, Fujimoto T, et al. Clinical utility of newly developed immunoassays for serum concentrations of adalimumab and anti-adalimumab antibodies in patients with Crohn’s disease. J Gastroenterol. 2014; 49:100–109. PMID: 23575576.
Article8. Imaeda H, Andoh A, Fujiyama Y. Development of a new immunoassay for the accurate determination of anti-infliximab antibodies in inflammatory bowel disease. J Gastroenterol. 2012; 47:136–143. PMID: 21953314.
Article9. Best WR, Becktel JM, Singleton JW, Kern F Jr. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology. 1976; 70:439–444. PMID: 1248701.10. Sou S, Matsui T, Yao T, et al. Clinical and endoscopic healing after infliximab treatment in patients with Crohn’s disease. Dig Endosc. 2006; 18:29–33.
Article11. Beppu T, Ono Y, Matsui T, et al. Mucosal healing of ileal lesions is associated with long-term clinical remission after infliximab maintenance treatment in patients with Crohn’s disease. Dig Endosc. 2015; 27:73–81. PMID: 24833527.
Article12. Imaeda H, Bamba S, Takahashi K, et al. Relationship between serum infliximab trough levels and endoscopic activities in patients with Crohn’s disease under scheduled maintenance treatment. J Gastroenterol. 2014; 49:674–682. PMID: 23666424.
Article13. Schnitzler F, Fidder H, Ferrante M, et al. Mucosal healing predicts long-term outcome of maintenance therapy with infliximab in Crohn’s disease. Inflamm Bowel Dis. 2009; 15:1295–1301. PMID: 19340881.
Article14. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance infliximab for Crohn's disease: the ACCENT I randomised trial. Lancet. 2002; 359:1541–1549. PMID: 12047962.
Article15. Ungar B, Levy I, Yavne Y, et al. Optimizing anti-TNF-alpha therapy: serum levels of infliximab and adalimumab are associated with mucosal healing in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2016; 14:550–557. PMID: 26538204.16. Roblin X, Marotte H, Leclerc M, et al. Combination of C-reactive protein, infliximab trough levels, and stable but not transient antibodies to infliximab are associated with loss of response to infliximab in inflammatory bowel disease. J Crohns Colitis. 2015; 9:525–531. PMID: 25895875.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Early Infliximab Trough Levels Predict the Long-term Efficacy of Infliximab in a Randomized Controlled Trial in Patients with Active Crohn’s Disease Comparing, between CT-P13 and Originator Infliximab
- Factors Affecting Surgical Treatment With Infliximab Therapy in Perianal Fistula With Crohn Disease
- Recent Trends of Infliximab Treatment for Crohn's Disease
- Adalimumab or infliximab: which is better for perianal fistula in Crohn's disease?
- A Case of Infliximab-induced Psoriasis in Treatment of Ankylosing Spondylitis
