Ann Pediatr Endocrinol Metab.
2017 Mar;22(1):1-5. 10.6065/apem.2017.22.1.1.
Bone modeling, remodeling, and skeletal health in children and adolescents: mineral accrual, assessment and treatment
- Affiliations
-
- 1Department of Health Sciences, University of Florence, Anna Meyer Children's University Hospital, Florence, Italy. stefano.stagi@yahoo.it
- KMID: 2409793
- DOI: http://doi.org/10.6065/apem.2017.22.1.1
Abstract
- The modeling and remodeling process of the bone is fundamental to maintaining its integrity and mechanical properties. Many physical and biochemical factors during childhood and adolescence are crucially important for the development of healthy bones. Systemic conditions, such as hormonal status, nutrition, physical inactivity, or many pharmacological treatments, as well as a local variation in the load, can influence bone turnover and, consequently, the attainment of a proper peak bone mass. However, many diseases affecting children and adolescents can be associated with a reduction in bone accrual or a loss of bone mass and quality, which leads to an increased risk of fracture over one's life. In this review, we examine the effects of genetics, physical activity, chronic diseases and pharmacological treatments, and dietary factors on bone integrity in children and adolescents. We also briefly describe the specific tools that are currently used in assessing bone health.
Keyword
MeSH Terms
Figure
-
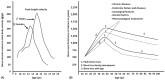
Fig. 1 (A) Growth of bone mass in relation to height growth velocity and difference in peak bone mass between males (♂) and females (♀). (B) Difference in peak bone mass between males (♂) and females (♀) and factors and diseases that influence the peak bone mass and the risk of osteopenia/osteoporosis in adulthood.
Cited by 1 articles
-
Factors affecting bone mineral density in children and adolescents with systemic lupus erythematosus
Su Jin Park, Soo Yeun Sim, Dae Chul Jeong, Byung-Kyu Suh, Moon Bae Ahn
Ann Pediatr Endocrinol Metab. 2024;29(3):191-200. doi: 10.6065/apem.2346060.030.
Reference
-
1. Javaid MK, Cooper C. Prenatal and childhood influences on osteoporosis. Best Pract Res Clin Endocrinol Metab. 2002; 16:349–367. PMID: 12064897.
Article2. Bachrach LK. Acquisition of optimal bone mass in childhood and adolescence. Trends Endocrinol Metab. 2001; 12:22–28. PMID: 11137037.
Article3. Carey DE, Golden NH. Bone health in adolescence. Adolesc Med State Art Rev. 2015; 26:291–325. PMID: 26999874.
Article4. Stagi S, Cavalli L, Iurato C, Seminara S, Brandi ML, de Martino M. Bone metabolism in children and adolescents: main characteristics of the determinants of peak bone mass. Clin Cases Miner Bone Metab. 2013; 10:172–179. PMID: 24554926.5. Mitchell JA, Cousminer DL, Zemel BS, Grant SF, Chesi A. Genetics of pediatric bone strength. Bonekey Rep. 2016; 5:823. PMID: 27579163.
Article6. Kambas A, Leontsini D, Avloniti A, Chatzinikolaou A, Stampoulis T, Makris K, et al. Physical activity may be a potent regulator of bone turnover biomarkers in healthy girls during preadolescence. J Bone Miner Metab. 2016; 11. 12. [Epub]. DOI: 10.1007/s00774-016-0794-3.
Article7. Gordon CM, Zemel BS, Wren TA, Leonard MB, Bachrach LK, Rauch F, et al. The determinants of peak bone mass. J Pediatr. 2017; 180:261–269. PMID: 27816219.
Article8. Ponrartana S, Aggabao PC, Hu HH, Aldrovandi GM, Wren TA, Gilsanz V. Brown adipose tissue and its relationship to bone structure in pediatric patients. J Clin Endocrinol Metab. 2012; 97:2693–2698. PMID: 22593587.
Article9. Bianchi ML, Baim S, Bishop NJ, Gordon CM, Hans DB, Langman CB, et al. Official positions of the International Society for Clinical Densitometry (ISCD) on DXA evaluation in children and adolescents. Pediatr Nephrol. 2010; 25:37–47. PMID: 19603190.
Article10. Stagi S, Cavalli L, Seminara S, de Martino M, Brandi ML. The ever-expanding conundrum of primary osteoporosis: aetiopathogenesis, diagnosis, and treatment. Ital J Pediatr. 2014; 40:55. PMID: 24906390.
Article11. von Scheven E, Corbin KJ, Stagi S, Cimaz R. Glucocorticoid-associated osteoporosis in chronic inflammatory diseases: epidemiology, mechanisms, diagnosis, and treatment. Curr Osteoporos Rep. 2014; 12:289–299. PMID: 25001898.
Article12. Vega D, Maalouf NM, Sakhaee K. Clinical review #: the role of receptor activator of nuclear factor-kappaB (RANK)/RANK ligand/osteoprotegerin: clinical implications. J Clin Endocrinol Metab. 2007; 92:4514–4521. PMID: 17895323.
Article13. Williams KM. Update on bone health in pediatric chronic disease. Endocrinol Metab Clin North Am. 2016; 45:433–441. PMID: 27241973.
Article14. Choudhary G, Gupta RK, Beniwal J. Bone mineral density in celiac disease. Indian J Pediatr. 2016; 12. 27. [Epub]. DOI: 10.1007/s12098-016-2273-1.
Article15. Carnevale V, Romagnoli E, D'Erasmo E. Skeletal involvement in patients with diabetes mellitus. Diabetes Metab Res Rev. 2004; 20:196–204. PMID: 15133750.
Article16. Galluzzi F, Stagi S, Salti R, Toni S, Piscitelli E, Simonini G, et al. Osteoprotegerin serum levels in children with type 1 diabetes: a potential modulating role in bone status. Eur J Endocrinol. 2005; 153:879–885. PMID: 16322394.
Article17. Khan TS, Fraser LA. Type 1 diabetes and osteoporosis: from molecular pathways to bone phenotype. J Osteoporos. 2015; 2015:174186. PMID: 25874154.
Article18. Wasserman H, O'Donnell JM, Gordon CM. Use of dual energy X-ray absorptiometry in pediatric patients. Bone. 2016; 12. 15. [Epub]. DOI: 10.1016/j.bone.2016.12.008.
Article19. Zemel BS, Kalkwarf HJ, Gilsanz V, Lappe JM, Oberfield S, Shepherd JA, et al. Revised reference curves for bone mineral content and areal bone mineral density according to age and sex for black and non-black children: results of the bone mineral density in childhood study. J Clin Endocrinol Metab. 2011; 96:3160–3169. PMID: 21917867.
Article20. Crabtree NJ, Arabi A, Bachrach LK, Fewtrell M, El-Hajj Fuleihan G, Kecskemethy HH, et al. Dual-energy X-ray absorptiometry interpretation and reporting in children and adolescents: the revised 2013 ISCD Pediatric Official Positions. J Clin Densitom. 2014; 17:225–242. PMID: 24690232.
Article21. Zemel BS. Quantitative computed tomography and computed tomography in children. Curr Osteoporos Rep. 2011; 9:284–290. PMID: 21968815.
Article22. Wang KC, Wang KC, Amirabadi A, Cheung E, Uleryk E, Moineddin R, et al. Evidence-based outcomes on diagnostic accuracy of quantitative ultrasound for assessment of pediatric osteoporosis - a systematic review. Pediatr Radiol. 2014; 44:1573–1587. PMID: 24962050.
Article23. Weeks BK, Hirsch R, Nogueira RC, Beck BR. Is calcaneal broadband ultrasound attenuation a valid index of dual-energy x-ray absorptiometry-derived bone mass in children? Bone Joint Res. 2016; 5:538–543. PMID: 27827803.
Article24. Cimaz R, Stagi S. Managing pediatric osteoporosis. Int J Clin Rheumatol. 2013; 8:509–512.
Article25. Zhang C, Liu Z, Klein GL. Overview of pediatric bone problems and related osteoporosis. J Musculoskelet Neuronal Interact. 2012; 12:174–182. PMID: 22947549.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bone morbidity in pediatric acute lymphoblastic leukemia
- Diagnosis and Management of Osteoporosis in Children and Adolescents
- School-based nutrition interventions can improve bone health in children and adolescents
- Emerging Anabolic Therapies for Osteoporosis
- Can Dental Cone Beam Computed Tomography Assess Bone Mineral Density?
