J Adv Prosthodont.
2018 Apr;10(2):79-84. 10.4047/jap.2018.10.2.79.
In-vitro performance and fracture strength of thin monolithic zirconia crowns
- Affiliations
-
- 1Head of Department of Postgraduate Education, Carolinum Dental University Institute gGmbH, Department of Prosthetic Dentistry, Goethe-University Frankfurt am Main, Frankfurt, Germany.
- 2Department of Prosthetic Dentistry, Faculty of Oral and Dental Medicine at JW Goethe-University Frankfurt am Main, Frankfurt, Germany.
- 3Department of Postgraduate Education, Faculty of Oral and Dental Medicine at JW Goethe-University Frankfurt am Main, Frankfurt, Germany.
- 4Department of Postgraduate Education, Carolinum Dental University Institute gGmbH, Department of Prosthetic Dentistry, Goethe-University Frankfurt am Main, Frankfurt, Germany.
- 5Head of Department of Prosthetic Dentistry, Carolinum Dental University Institute gGmbH, Department of Prosthetic Dentistry, Goethe-University Frankfurt am Main, Frankfurt, Germany.
- 6Department of Prosthetic Dentistry, UKR University Hospital Regensburg, Regensburg, Germany. martin.rosentritt@ukr.de
- KMID: 2409626
- DOI: http://doi.org/10.4047/jap.2018.10.2.79
Abstract
- PURPOSE
All-ceramic restorations required extensive tooth preparation. The purpose of this in vitro study was to investigate a minimally invasive preparation and thickness of monolithic zirconia crowns, which would provide sufficient mechanical endurance and strength.
MATERIALS AND METHODS
Crowns with thickness of 0.2 mm (group 0.2, n=32) or of 0.5 mm (group 0.5, n=32) were milled from zirconia and fixed with resin-based adhesives (groups 0.2A, 0.5A) or zinc phosphate cements (groups 0.2C, 0.5C). Half of the samples in each subgroup (n=8) underwent thermal cycling and mechanical loading (TCML)(TC: 5℃ and 55℃, 2×3,000 cycles, 2 min/cycle; ML: 50 N, 1.2×106 cycles), while the other samples were stored in water (37℃/24 h). Survival rates were compared (Kaplan-Maier). The specimens surviving TCML were loaded to fracture and the maximal fracture force was determined (ANOVA; Bonferroni; α=.05). The fracture mode was analyzed.
RESULTS
In both 0.5 groups, all crowns survived TCML, and the comparison of fracture strength among crowns with and without TCML showed no significant difference (P=.628). Four crowns in group 0.2A and all of the crowns in group 0.2C failed during TCML. The fracture strength after 24 hours of the cemented 0.2 mm-thick crowns was significantly lower than that of adhesive bonded crowns. All cemented crowns provided fracture in the crown, while about 80% of the adhesively bonded crowns fractured through crown and die.
CONCLUSION
0.5 mm thick monolithic crowns possessed sufficient strength to endure physiologic performance, regardless of the type of cementation. Fracture strength of the 0.2 mm cemented crowns was too low for clinical application.
Keyword
MeSH Terms
Figure
-

Fig. 1 Specimen example (zirconia crowns and artificial tooth).
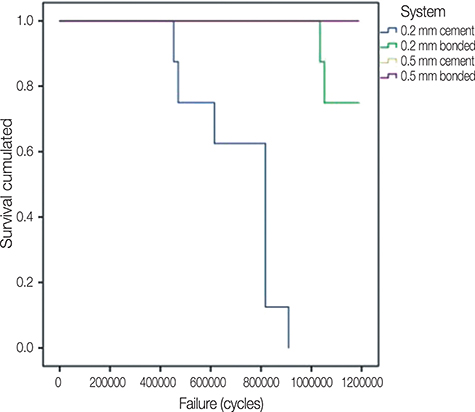
Fig. 2 Cumulated survival during TCML; 0.5 bonded and cemented crowns showed no failures.
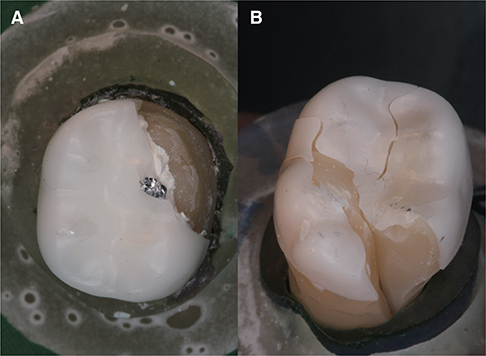
Fig. 3 Fracture pattern. (A) fracture of the crown, (B) fracture through crown and tooth.
Cited by 1 articles
-
Retrospective clinical and radiographic evaluation of restored endodontically treated teeth
Paula Pontes Garcia, Aline Cappoani, Ricardo Susin Schelbauer, Gisele Maria Correr, Carla Castiglia Gonzaga
Restor Dent Endod. 2020;45(4):e49. doi: 10.5395/rde.2020.45.e49.
Reference
-
1. Kelly JR, Nishimura I, Campbell SD. Ceramics in dentistry: historical roots and current perspectives. J Prosthet Dent. 1996; 75:18–32.
Article2. Rimmer S. Modern dental ceramics: An overview. Int Dent SA. 2006; 8:32–39.3. Griggs JA. Recent advances in materials for all-ceramic restorations. Dent Clin North Am. 2007; 51:713–727.
Article4. Piconi C, Maccauro G. Zirconia as a ceramic biomaterial. Biomaterials. 1999; 20:1–25.
Article5. Sorrentino R, De Simone G, Tetè S, Russo S, Zarone F. Five-year prospective clinical study of posterior three-unit zirconia-based fixed dental prostheses. Clin Oral Investig. 2012; 16:977–985.
Article6. Schmitter M, Mueller D, Rues S. Chipping behaviour of all-ceramic crowns with zirconia framework and CAD/CAM manufactured veneer. J Dent. 2012; 40:154–162.
Article7. Kirmali O, Akin H, Ozdemir AK. Shear bond strength of veneering ceramic to zirconia core after different surface treatments. Photomed Laser Surg. 2013; 31:261–268.
Article8. Choi YS, Kim SH, Lee JB, Han JS, Yeo IS. In vitro evaluation of fracture strength of zirconia restoration veneered with various ceramic materials. J Adv Prosthodont. 2012; 4:162–169.9. Sundh A, Molin M, Sjögren G. Fracture resistance of yttrium oxide partially-stabilized zirconia all-ceramic bridges after veneering and mechanical fatigue testing. Dent Mater. 2005; 21:476–482.
Article10. Wimmer T, Hostettler J, Beuer F, Stawarczyk B. Load-bearing capacity of soldered and subsequently veneered 4-unit zirconia FDPs. J Mech Behav Biomed Mater. 2013; 23:1–7.
Article11. Guess PC, Bonfante EA, Silva NR, Coelho PG, Thompson VP. Effect of core design and veneering technique on damage and reliability of Y-TZP-supported crowns. Dent Mater. 2013; 29:307–316.
Article12. Preis V, Letsch C, Handel G, Behr M, Schneider-Feyrer S, Rosentritt M. Influence of substructure design, veneer application technique, and firing regime on the in vitro performance of molar zirconia crowns. Dent Mater. 2013; 29:e113–e121.
Article13. Zhang Y, Mai Z, Barani A, Bush M, Lawn B. Fracture-resistant monolithic dental crowns. Dent Mater. 2016; 32:442–449.
Article14. Zhang Y, Lee JJ, Srikanth R, Lawn BR. Edge chipping and flexural resistance of monolithic ceramics. Dent Mater. 2013; 29:1201–1208.
Article15. Lameira DP, Buarque e, Andrade e Silva F, De Souza GM. Fracture strength of aged monolithic and bilayer zirconia-based crowns. Biomed Res Int. 2015; 2015:418641.
Article16. Nordahl N, Vult von Steyern P, Larsson C. Fracture strength of ceramic monolithic crown systems of different thickness. J Oral Sci. 2015; 57:255–261.
Article17. Thompson VP, Rekow DE. Dental ceramics and the molar crown testing ground. J Appl Oral Sci. 2004; 12:26–36.
Article18. Nakamura K, Harada A, Inagaki R, Kanno T, Niwano Y, Milleding P, Örtengren U. Fracture resistance of monolithic zirconia molar crowns with reduced thickness. Acta Odontol Scand. 2015; 73:602–608.
Article19. Nakamura K, Mouhat M, Nergård JM, Lægreid SJ, Kanno T, Milleding P, Örtengren U. Effect of cements on fracture resistance of monolithic zirconia crowns. Acta Biomater Odontol Scand. 2016; 2:12–19.
Article20. Sorrentino R, Triulzio C, Tricarico MG, Bonadeo G, Gherlone EF, Ferrari M. In vitro analysis of the fracture resistance of CAD-CAM monolithic zirconia molar crowns with different occlusal thickness. J Mech Behav Biomed Mater. 2016; 61:328–333.
Article21. Sun T, Zhou S, Lai R, Liu R, Ma S, Zhou Z, Longquan S. Load-bearing capacity and the recommended thickness of dental monolithic zirconia single crowns. J Mech Behav Biomed Mater. 2014; 35:93–101.
Article22. Papia E, Larsson C, du Toit M, Vult von. Bonding between oxide ceramics and adhesive cement systems: a systematic review. J Biomed Mater Res B Appl Biomater. 2014; 102:395–413.
Article23. Kelly JR. Clinically relevant approach to failure testing of all-ceramic restorations. J Prosthet Dent. 1999; 81:652–661.
Article24. Rosentritt M, Behr M, Scharnagl P, Handel G, Kolbeck C. Influence of resilient support of abutment teeth on fracture resistance of all-ceramic fixed partial dentures: an in vitro study. Int J Prosthodont. 2011; 24:465–468.25. Rosentritt M, Behr M, Gebhard R, Handel G. Influence of stress simulation parameters on the fracture strength of all-ceramic fixed-partial dentures. Dent Mater. 2006; 22:176–182.
Article26. Rosentritt M, Behr M, van der Zel JM, Feilzer AJ. Approach for valuating the influence of laboratory simulation. Dent Mater. 2009; 25:348–352.
Article27. Rosentritt M, Siavikis G, Behr M, Kolbeck C, Handel G. Approach for valuating the significance of laboratory simulation. J Dent. 2008; 36:1048–1053.
Article28. Rosentritt M, Steiger D, Behr M, Handel G, Kolbeck C. Influence of substructure design and spacer settings on the in vitro performance of molar zirconia crowns. J Dent. 2009; 37:978–983.
Article29. Rosentritt M, Behr M, Thaller C, Rudolph H, Feilzer A. Fracture performance of computer-aided manufactured zirconia and alloy crowns. Quintessence Int. 2009; 40:655–662.30. Rosentritt M, Plein T, Kolbeck C, Behr M, Handel G. In vitro fracture force and marginal adaptation of ceramic crowns fixed on natural and artificial teeth. Int J Prosthodont. 2000; 13:387–391.31. Beuer F, Stimmelmayr M, Gueth JF, Edelhoff D, Naumann M. In vitro performance of full-contour zirconia single crowns. Dent Mater. 2012; 28:449–456.
Article32. Rekow ED, Harsono M, Janal M, Thompson VP, Zhang G. Factorial analysis of variables influencing stress in all-ceramic crowns. Dent Mater. 2006; 22:125–132.
Article33. Gehrt M, Wolfart S, Rafai N, Reich S, Edelhoff D. Clinical results of lithium-disilicate crowns after up to 9 years of service. Clin Oral Investig. 2013; 17:275–284.
Article34. Rauch A, Reich S, Schierz O. Chair-side generated posterior monolithic lithium disilicate crowns: clinical survival after 6 years. Clin Oral Investig. 2017; 21:2083–2089.35. Ha SR. Biomechanical three-dimensional finite element analysis of monolithic zirconia crown with different cement type. J Adv Prosthodont. 2015; 7:475–483.
Article36. Ma L, Guess PC, Zhang Y. Load-bearing properties of minimal-invasive monolithic lithium disilicate and zirconia occlusal onlays: finite element and theoretical analyses. Dent Mater. 2013; 29:742–751.
Article37. Stawarczyk B, Beuer F, Ender A, Roos M, Edelhoff D, Wimmer T. Influence of cementation and cement type on the fracture load testing methodology of anterior crowns made of different materials. Dent Mater J. 2013; 32:888–895.
Article38. Al-Wahadni AM, Hussey DL, Grey N, Hatamleh MM. Fracture resistance of aluminium oxide and lithium disilicate-based crowns using different luting cements: an in vitro study. J Contemp Dent Pract. 2009; 10:51–58.
Article39. Vult von Steyern P, Ebbesson S, Holmgren J, Haag P, Nilner K. Fracture strength of two oxide ceramic crown systems after cyclic pre-loading and thermocycling. J Oral Rehabil. 2006; 33:682–689.
Article40. Raadsheer MC, van Eijden TM, van Ginkel FC, Prahl-Andersen B. Contribution of jaw muscle size and craniofacial morphology to human bite force magnitude. J Dent Res. 1999; 78:31–42.
Article41. Bindl A, Lüthy H, Mörmann WH. Strength and fracture pattern of monolithic CAD/CAM-generated posterior crowns. Dent Mater. 2006; 22:29–36.
Article42. Varga S, Spalj S, Lapter Varga M, Anic Milosevic S, Mestrovic S, Slaj M. Maximum voluntary molar bite force in subjects with normal occlusion. Eur J Orthod. 2011; 33:427–433.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fracture strength of zirconia monolithic crowns and metal-ceramic crowns after cyclic loading and thermocycling
- Fracture strength of zirconia monolithic crowns
- Fracture resistance of implant- supported monolithic crowns cemented to zirconia hybrid-abutments: zirconia-based crowns vs. lithium disilicate crowns
- Influence of the preparation design and artificial aging on the fracture resistance of monolithic zirconia crowns
- Esthetic anterior restoration using 3M Lavaâ„¢ Esthetic monolithic zirconia
