Angle Closure and the Acute Rise of Intraocular Pressure after Administration of Methazolamide
- Affiliations
-
- 1Department of Ophthalmology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. brio17@naver.com
- 2Asan City Health Center, Asan, Korea.
- KMID: 2397858
- DOI: http://doi.org/10.3341/jkos.2017.58.12.1420
Abstract
- PURPOSE
To report a case involving an unexpected increase in intraocular pressure (IOP) and acute angle closure after oral administration of methazolamide.
CASE SUMMARY
A 38-year-old male visited the emergency department complaining of decreased visual acuity (VA) and ocular pain. These symptoms developed after he took two tablets of 50 mg methazolamide because his IOP was above normal after a short course of systemic steroid treatment. His uncorrected VA dropped to 0.04 and the refractive error was −6.5 diopters in both eyes. The anterior chamber was very shallow, and the IOPs were 46 mmHg in the right eye and 42 mmHg in the left eye. Macular retinal folds were observed in both eyes in infrared fundus images. The patient was instructed not to take methazolamide, which was suspected as the cause of this idiosyncratic drug reaction. He was prescribed topical anti-glaucoma medications and cycloplegics to relieve the acute angle closure, and all symptoms disappeared after these treatments.
CONCLUSIONS
Methazolamide is a sulfa derivative like topiramate, which can cause acute angle closure involving edema of the ciliary body and anterior displacement of the lens-iris diaphragm. Clinicians should consider this possible IOP increase before prescribing methazolamide.
Keyword
MeSH Terms
Figure
-

Figure 1 Scheimpflug images of AL-scan® (Nidek, Gamagori, Japan). (A) Shallow central anterior chamber at the initial presentation. (B) Deepening of central anterior chamber at the final visit. ACD = anterior chamber depth, distance between the anterior corneal surface to the anterior lens surface; CCT = central corneal thickness; OD = oculus dexter; OS = oculus sinister.

Figure 2 Anterior segment optical coherent tomography of temporal quadrant of drainage angle in the right eye. Peripheral crowding of angle was shown in (A) (2 days after acute angle closure). Drainage angle has been widened, but peripheral iris was still located more anteriorly than central iris (B) (4 days after acute angle closure).
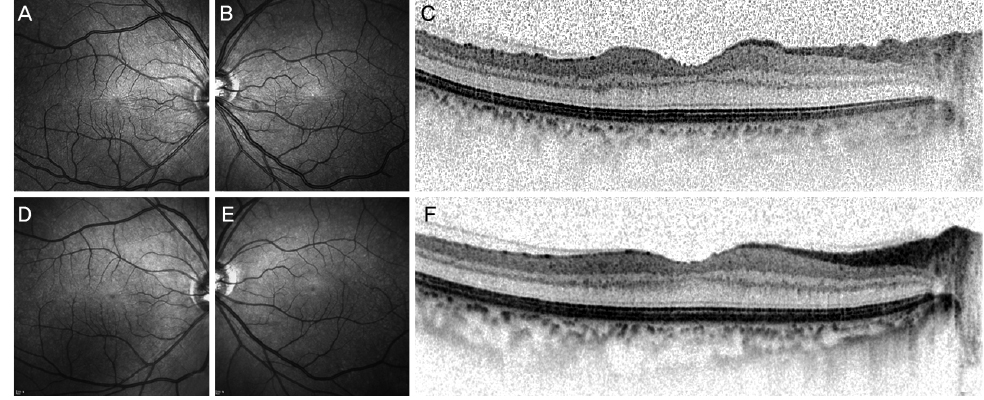
Figure 3 Infrared (IR) images and optical coherent tomography (OCT) images. IR images (A, B, D, E) and OCT images of the right eye taken simultaneously with A and D (C, F). IR images showed that retinal folds at the initial presentation (A, B), and resolution of retinal folds at the final visit (D, E). OCT images showed that retinal folds were limited in the inner retinal layers (A), and resolved at the final visit (F).
Reference
-
1. Lee GC, Tam CP, Danesh-Meyer HV, et al. Bilateral angle closure glaucoma induced by sulphonamide-derived medications. Clin Exp Ophthalmol. 2007; 35:55–58.2. Panday VA, Rhee DJ. Review of sulfonamide-induced acute myopia and acute bilateral angle-closure glaucoma. Compr Ophthalmol Update. 2007; 8:271–276.3. Korol' EA. Transitory myopia in combination with transitory glaucoma. Zdravookhr Beloruss. 1962; 8:66–67.4. Jeon C, Kee CW. Topiramate-induced acute angle-closure glaucoma. J Korean Ophthalmol Soc. 2005; 46:1944–1950.5. Craig JE, Ong TJ, Louis DL, Wells JM. Mechanism of topiramate-induced acute-onset myopia and angle closure glaucoma. Am J Ophthalmol. 2004; 137:193–195.6. Fraunfelder FW, Fraunfelder FT, Keates EU. Topiramate-associated acute, bilateral, secondary angle-closure glaucoma. Ophthalmology. 2004; 111:109–111.7. Bovino JA, Marcus DF. The mechanism of transient myopia induced by sulfonamide therapy. Am J Ophthalmol. 1982; 94:99–102.8. Krieg PH, Schipper I. Drug-induced ciliary body oedema: a new theory. Eye (Lond). 1996; 10:121–126.9. Sen HA, O'Halloran HS, Lee WB. Case reports and small case series: topiramate-induced acute myopia and retinal striae. Arch Ophthalmol. 2001; 119:775–777.10. Ryan EH Jr, Jampol LM. Drug-induced acute transient myopia with retinal folds. Retina. 1986; 6:220–223.11. Gualtieri W, Janula J. Topiramate maculopathy. Int Ophthalmol. 2013; 33:103–106.12. Natesh S, Rajashekhara SK, Rao AS, Shetty B. Topiramate-induced angle closure with acute myopia, macular striae. Oman J Ophthalmol. 2010; 3:26–28.13. Kwon SJ, Park DH, Shin JP. Bilateral transient myopia, angle-closure glaucoma, and choroidal detachment induced by methazolamide. Jpn J Ophthalmol. 2012; 56:515–517.14. Aref AA, Sayyad FE, Ayres B, Lee RK. Acute bilateral angle closure glaucoma induced by methazolamide. Clin Ophthalmol. 2013; 7:279–282.15. Abramson DH, Coleman DJ, Forbes M, Franzen LA. Pilocarpine. Effect on the anterior chamber and lens thickness. Arch Ophthalmol. 1972; 87:615–620.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Iridoshisis with Angle Closure Glaucoma
- Effect of Apraclonidine Hydrochloride on the Acute Intraocular Pressure Rise after Argon laser Iridotomy
- Long-term Intraocular Pressure Elevation after Primary Angle Closure Treated with Early Phacoemulsification
- Four cases of Stevens-Johnson Syndrome associated with Methazolamide Treatment
- Epidermal Necrolysis due to Methazolamide Treatment in Glaucomatous Patients
