Ann Pediatr Endocrinol Metab.
2017 Sep;22(3):203-207. 10.6065/apem.2017.22.3.203.
An atypical case of Noonan syndrome with KRAS mutation diagnosed by targeted exome sequencing
- Affiliations
-
- 1Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. nadri1217@naver.com
- 2Green Cross Laboratories, Green Cross Genome, Yongin, Korea.
- 3Department of Pediatrics, Inha University Hospital, Inha University Graduate School of Medicine, Incheon, Korea.
- KMID: 2396141
- DOI: http://doi.org/10.6065/apem.2017.22.3.203
Abstract
- Noonan syndrome (NS) is a genetic disorder caused by autosomal dominant inheritance and is characterized by a distinctive facial appearance, short stature, chest deformity, and congenital heart disease. In individuals with NS, germline mutations have been identified in several genes involved in the RAS/mitogen-activated protein kinase signal transduction pathway. Because of its clinical and genetic heterogeneity, the conventional diagnostic protocol with Sanger sequencing requires a multistep approach. Therefore, molecular genetic diagnosis using targeted exome sequencing (TES) is considered a less expensive and faster method, particularly for patients who do not fulfill the clinical diagnostic criteria of NS. In this case, the patient showed short stature, dysmorphic facial features suggestive of NS, feeding intolerance, cryptorchidism, and intellectual disability in early childhood. At the age of 16, the patient still showed extreme short stature with delayed puberty and characteristic facial features suggestive of NS. Although the patient had no cardiac problems or chest wall deformities, which are commonly present in NS and are major concerns for patients and clinicians, the patient showed several other characteristic clinical features of NS. Considering the possibility of a genetic disorder, including NS, a molecular genetic study with TES was performed. With TES analysis, we detected a pathogenic variant of c.458A > T in KRAS in this patient with atypical NS phenotype and provided appropriate clinical management and genetic counseling. The application of TES enables accurate molecular diagnosis of patients with nonspecific or atypical features in genetic diseases with several responsible genes, such as NS.
MeSH Terms
-
Congenital Abnormalities
Cryptorchidism
Diagnosis
Exome*
Genetic Counseling
Genetic Heterogeneity
Germ-Line Mutation
Heart Defects, Congenital
Humans
Intellectual Disability
Male
Methods
Molecular Biology
Noonan Syndrome*
Phenotype
Protein Kinases
Puberty, Delayed
Signal Transduction
Thoracic Wall
Thorax
Wills
Protein Kinases
Figure
-
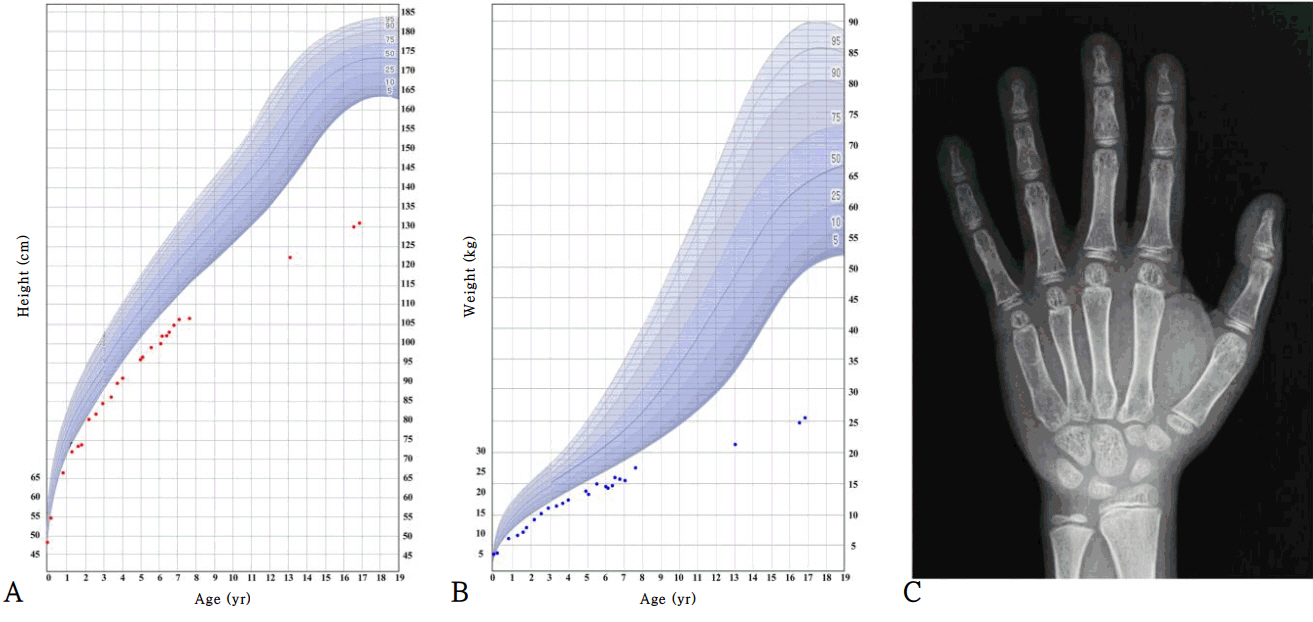
Fig. 1. Growth curve of patient with Noonan syndrome and X-ray of the left hand of patient at 16 years of age. Height (A), weight (B), and X-ray of left hand (C). The growth curve shows the severe growth retardation of the patient. At the age of 6 years, he was treated with growth hormone for 6 months. His bone maturation at age 16 was delayed (the standard bone age is 10 years for a male according to the Greulich and Pyle atlas).
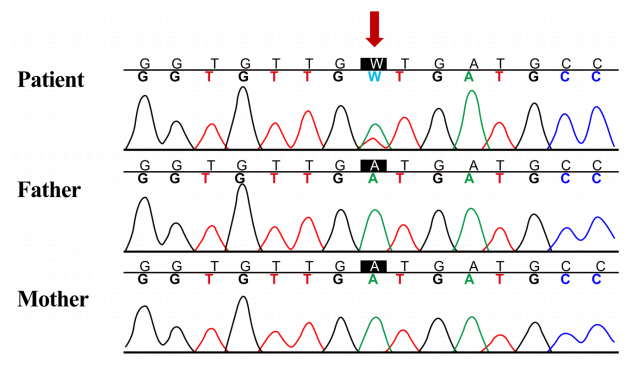
Fig. 2. Sanger sequencing confirmation of heterozygous mutation of KRAS. Heterozygous de novo mutation of c.458A > T (p.D153V) in exon 5 of KRAS was found by targeted exome sequencing and was confirmed by Sanger sequencing analysis (reference sequence: NM_004985.4).
Reference
-
References
1. Romano AA, Allanson JE, Dahlgren J, Gelb BD, Hall B, Pierpont ME, et al. Noonan syndrome: clinical features, diagnosis, and management guidelines. Pediatrics. 2010; 126:746–59.
Article2. Schubbert S, Zenker M, Rowe SL, Böll S, Klein C, Bollag G, et al. Germline KRAS mutations cause Noonan syndrome. Nat Genet. 2006; 38:331–6.
Article3. Ko JM, Kim JM, Kim GH, Yoo HW. PTPN11, SOS1, KRAS, and RAF1 gene analysis, and genotype-phenotype correlation in Korean patients with Noonan syndrome. J Hum Genet. 2008; 53:999–1006.
Article4. van der Burgt I, Berends E, Lommen E, van Beersum S, Hamel B, Mariman E. Clinical and molecular studies in a large Dutch family with Noonan syndrome. Am J Med Genet. 1994; 53:187–91.
Article5. Allanson JE, Bohring A, Dörr HG, Dufke A, Gillessen-Kaesbach G, Horn D, et al. The face of Noonan syndrome: Does phenotype predict genotype. Am J Med Genet A. 2010; 152A:1960–6.
Article6. Tartaglia M, Mehler EL, Goldberg R, Zampino G, Brunner HG, Kremer H, et al. Mutations in PTPN11, encoding the protein tyrosine phosphatase SHP-2, cause Noonan syndrome. Nat Genet. 2001; 29:465–8.
Article7. Lepri FR, Scavelli R, Digilio MC, Gnazzo M, Grotta S, Dentici ML, et al. Diagnosis of Noonan syndrome and related disorders using target next generation sequencing. BMC Med Genet. 2014; 15:14.
Article8. Aoki Y, Niihori T, Inoue S, Matsubara Y. Recent advances in RASopathies. J Hum Genet. 2016; 61:33–9.
Article9. Zenker M, Lehmann K, Schulz AL, Barth H, Hansmann D, Koenig R, et al. Expansion of the genotypic and phenotypic spectrum in patients with KRAS germline mutations. J Med Genet. 2007; 44:131–5.
Article10. Lim JS, Hwang JS, Lee JA, Kim DH, Park KD, Cheon GJ, et al. Bone mineral density according to age, bone age, and pubertal stages in korean children and adolescents. J Clin Densitom. 2010; 13:68–76.
Article11. Zenker M, Buheitel G, Rauch R, Koenig R, Bosse K, Kress W, et al. Genotype-phenotype correlations in Noonan syndrome. J Pediatr. 2004; 144:368–74.
Article12. Seaver LH, Irons M; American College of Medical Genetics (ACMG) Professional Practice and Guidelines Committee. ACMG practice guideline: genetic evaluation of short stature. Genet Med. 2009; 11:465–70.
Article13. Dauber A, Rosenfeld RG, Hirschhorn JN. Genetic evaluation of short stature. J Clin Endocrinol Metab. 2014; 99:3080–92.
Article14. Şıklar Z, Berberoğlu M. Syndromic disorders with short stature. J Clin Res Pediatr Endocrinol. 2014; 6:1–8.
Article15. Lisi EC, Cohn RD. Genetic evaluation of the pediatric patient with hypotonia: perspective from a hypotonia specialty clinic and review of the literature. Dev Med Child Neurol. 2011; 53:586–99.
Article16. Niihori T, Aoki Y, Narumi Y, Neri G, Cavé H, Verloes A, et al. Germline KRAS and BRAF mutations in cardio-faciocutaneous syndrome. Nat Genet. 2006; 38:294–6.
Article17. Shaw AC, Kalidas K, Crosby AH, Jeffery S, Patton MA. The natural history of Noonan syndrome: a long-term followup study. Arch Dis Child. 2007; 92:128–32.
Article18. George CD, Patton MA, el Sawi M, Sharland M, Adam EJ. Abdominal ultrasound in Noonan syndrome: a study of 44 patients. Pediatr Radiol. 1993; 23:316–8.
Article19. Kim SW, Park SE, Jeong IH, Yoon JW, Lee CA, Jeon JH. Noonan syndrome confirmed to KRAS gene mutation: a case of KRAS gene mutation. J Korean Soc Neonatol. 2011; 18:374–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noonan Syndrome Confirmed to KRAS Gene Mutation: A Case of KRAS Gene Mutation
- A case of Noonan syndrome diagnosed using the facial recognition software (FACE2GENE)
- Exome Sequencing in Mendelian Disorders
- The first Korean case with Floating-Harbor syndrome with a novel SRCAP mutation diagnosed by targeted exome sequencing
- Identification of Two Cases of Ciliopathy-Associated Diabetes and Their Mutation Analysis Using Whole Exome Sequencing
