J Rheum Dis.
2011 Jun;18(2):118-121.
Efficacy of Imatinib Mesylate Treatment for a Patient with Rheumatoid Arthritis and Who Developed Chronic Myelogenous Leukemia
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea. antibio1004@hanmail.net
- 2Department of Laboratory Medicine, Pusan National University School of Medicine, Busan, Korea.
Abstract
- Rheumatoid arthritis is associated with an increased risk of hematological malignancy as a result of the RA itself or its treatment. We report here on an unusual case of a 55-year-old female with long-standing rheumatoid arthritis and who was treated with low dose methotrexate and hydrochloroquine. She was diagnosed with chronic myelogenous leukemia that manifested with severe thrombocytosis and basophilia, and this was treated with imatinib mesylate. After 6 months, she achieved a complete cytogenetic response of the CML and a complete resolution of all the RA symptoms without DMARDs.
MeSH Terms
-
Antirheumatic Agents
Arthritis, Rheumatoid
Benzamides
Cytogenetics
Female
Hematologic Neoplasms
Humans
Leukemia, Myelogenous, Chronic, BCR-ABL Positive
Mesylates
Methotrexate
Middle Aged
Piperazines
Pyrimidines
Thrombocytosis
Imatinib Mesylate
Antirheumatic Agents
Benzamides
Mesylates
Methotrexate
Piperazines
Pyrimidines
Figure
-

Figure 1. The X rays of both hands show bony erosion and ankylosis on both radiocarpal joints.

Figure 2. BM aspiration: The aspirate smear of the marrow and the touch preparation of the biopsy show mildly hypercellular marrow with a marked proliferation of dysplastic megakaryocytes (arrow) and many platelet clumpings (arrowhead). The blasts and pronormoblasts are mildly increased in number.
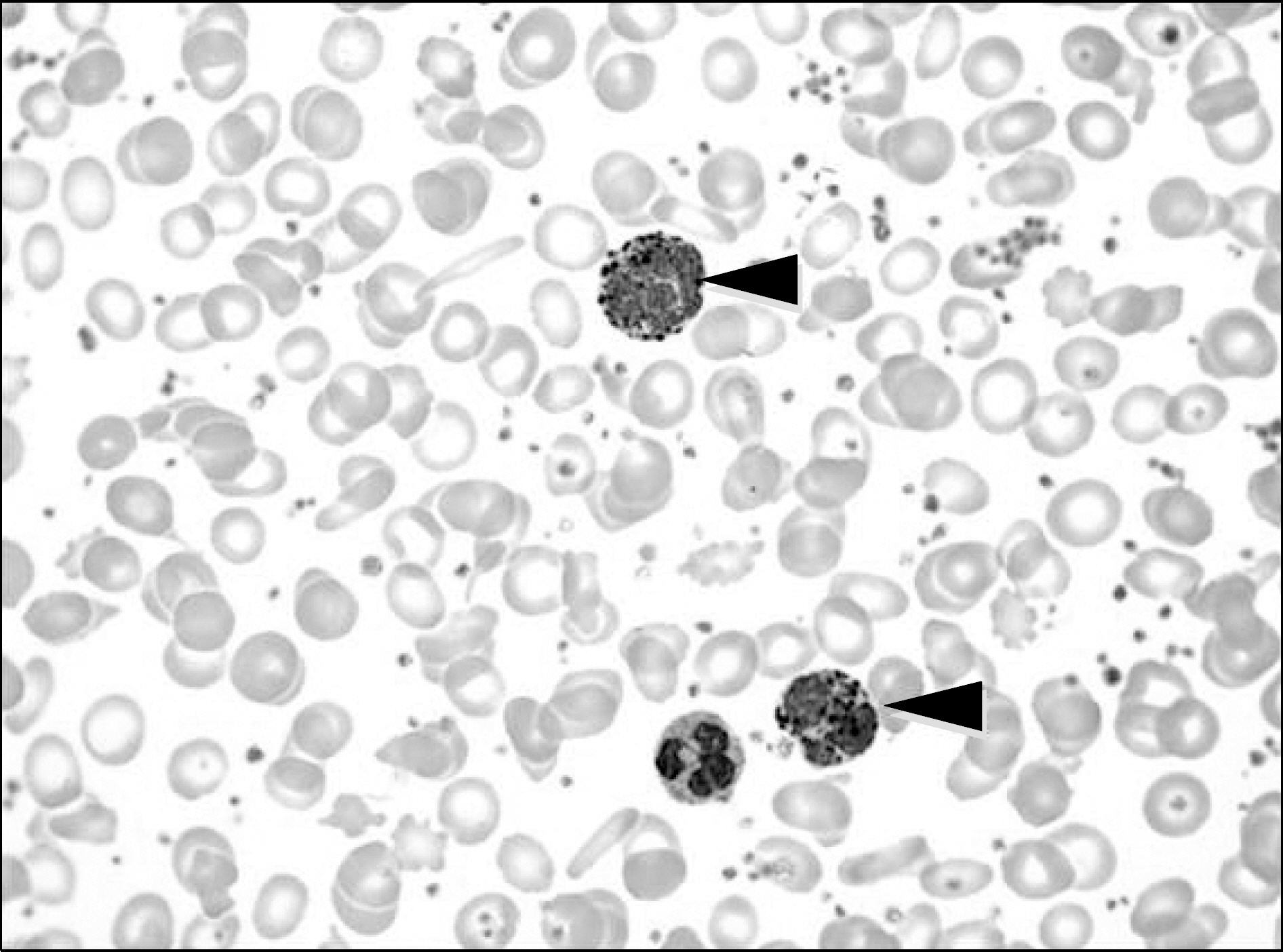
Figure 3. Peripheral blood: The erythrocytes reveal moderate microcytic hypochromic anemia with mild anisocytosis and poikilocytosis. The WBCs are mildly increased with marked basophilia (26%, arrowhead). The platelets are markedly increased in number with many platelet clumpings.
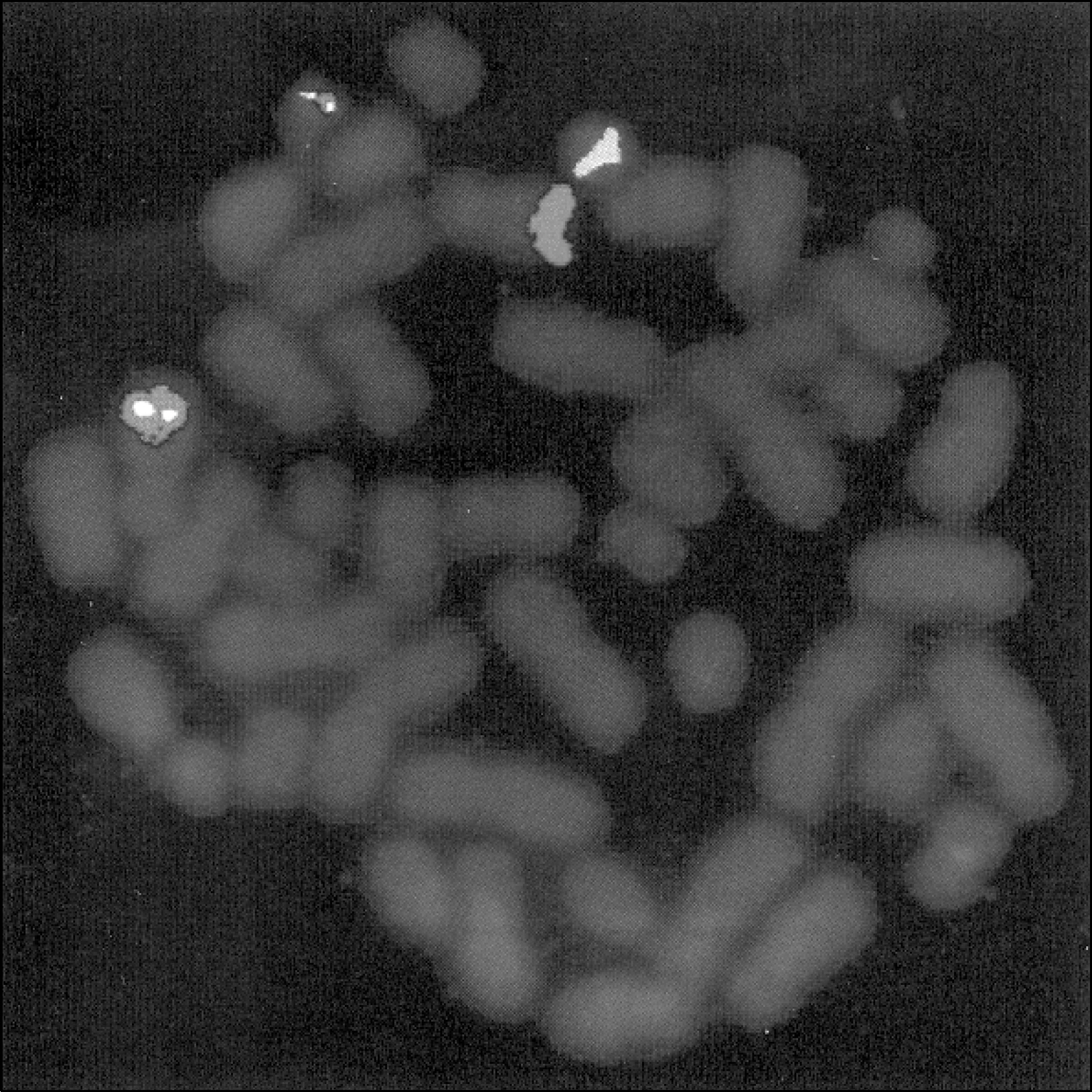
Figure 4. Positive BCR/ABL1 gene rearrangement FISH.
Reference
-
References
1. Williams WV, VonFeldt JM, Ramanujam T, Weiner DB. Tyrosine kinase signal transduction in rheumatoid synovitis. Semin Arthritis Rheum. 1992; 21:317–29.
Article2. Askling J, Fored CM, Baecklund E, Brandt L, Backlin C, Ekbom A, et al. Haematopoietic malignancies in rheumatoid arthritis: lymphoma risk and characteristics after exposure to tumour necrosis factor antagonists. Ann Rheum Dis. 2005; 64:1414–20.
Article3. Bernatsky S, Clarke AE, Suissa S. Hematologic malig-nant neoplasms after drug exposure in rheumatoid arthritis. Arch Intern Med. 2008; 168:378–81.
Article4. Asten P, Barrett J, Symmons D. Risk of developing cer- tain malignancies is related to duration of immunosuppressive drug exposure in patients with rheumatic diseases. J Rheumatol. 1999; 26:1705–14.5. Baker GL, Kahl LE, Zee BC, Stolzer BL, Agarwal AK, Medsger TA Jr. Malignancy following treatment of rheumatoid arthritis with cyclophosphamide. Longterm case-control followup study. Am J Med. 1987; 83:1–9.6. Wolfe F, Michaud K. Lymphoma in rheumatoid arthritis: the effect of methotrexate and antitumor necrosis factor therapy in 18,572 patients. Arthritis Rheum. 2004; 50:1740–51.
Article7. Pointud P, Prudat M, Peron JM. Acute leukemia after low dose methotrexate therapy in a patient with rheumatoid arthritis. J Rheumatol. 1993; 20:1215–6.8. Georgescu L, Quinn GC, Schwartzman S, Paget SA. Lymphoma in patients with rheumatoid arthritis: association with the disease state or methotrexate treatment. Semin Arthritis Rheum. 1997; 26:794–804.9. Cibere J, Sibley J, Haga M. Rheumatoid arthritis and the risk of malignancy. Arthritis Rheum. 1997; 40:1580–6.
Article10. Piper H, Mulherin D, Hardwick N. Multiple haemato-logical malignancies in a patient with rheumatoid arthritis without exposure to disease modifying therapy. Ann Rheum Dis. 2006; 65:268–9.
Article11. D'Aura Swanson C, Paniagua RT, Lindstrom TM, Robinson WH. Tyrosine kinases as targets for the treatment of rheumatoid arthritis. Nat Rev Rheumatol. 2009; 5:317–24.12. Kameda H, Ishigami H, Suzuki M, Abe T, Takeuchi T. Imatinib mesylate inhibits proliferation of rheumatoid synovial fibroblast-like cells and phosphorylation of Gab adapter proteins activated by platelet-derived growth factor. Clin Exp Immunol. 2006; 144:335–41.
Article13. Ando W, Hashimoto J, Nampei A, Tsuboi H, Tateishi K, Ono T, et al. Imatinib mesylate inhibits osteoclastogenesis and joint destruction in rats with collagen-induced arthritis (CIA). J Bone Miner Metab. 2006; 24:274–82.
Article14. Miyachi K, Ihara A, Hankins RW, Murai R, Maehiro S, Miyashita H. Efficacy of imatinib mesylate (STI571) treatment for a patient with rheumatoid arthritis developing chronic myelogenous leukemia. Clin Rheumatol. 2003; 22:329–32.
Article15. Eklund KK, Joensuu H. Treatment of rheumatoid arthritis with imatinib mesylate: clinical improvement in three refractory cases. Ann Med. 2003; 35:362–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imatinib Mesylate is Effective for Patients Not Only with Chronic Myeloid Leukemia, but Also Rheumatoid Arthritis
- Reversal of Marrow Fibrosis Following Imatinib Mesylate Therapy in a Patient with Chronic Myelogenous Leukemia Who Was Refractory to Interferon-alpha
- Pityriasis rosea-like Drug Eruption Induced by Imatinib Mesylate (Gleevec(TM))
- Peripheral neuropathy associated with imatinib therapy for chronic myeloid leukemia
- A Case of Psoriasiform Drug Eruption Induced by Imatinib Mesylate (GleevecTM)
