Baseline Cardiovascular Characteristics of Adult Patients with Chronic Kidney Disease from the KoreaN Cohort Study for Outcomes in Patients With Chronic Kidney Disease (KNOW-CKD)
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. hansh@yuhs.ac
- 2Department of Internal Medicine, Seoul National University, Seoul, Korea.
- 3Medical Research Collaborating Center, Seoul National University Hospital and Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea.
- 5Department of Internal Medicine, Inje University, Pusan Paik Hospital, Busan, Korea.
- 6Department of Internal Medicine, Eulji Medical Center, Eulji University, Seoul, Korea.
- KMID: 2364166
- DOI: http://doi.org/10.3346/jkms.2017.32.2.231
Abstract
- Cardiovascular disease (CVD) is the most common cause of death in patients with chronic kidney disease (CKD). We report the baseline cardiovascular characteristics of 2,238 participants by using the data of the KoreaN Cohort Study for Outcomes in Patients With Chronic Kidney Disease (KNOW-CKD) study. The cohort comprises 5 subcohorts according to the cause of CKD: glomerulonephritis (GN), diabetic nephropathy (DN), hypertensive nephropathy (HTN), polycystic kidney disease (PKD), and unclassified. The average estimated glomerular filtration rate (eGFR) was 50.5 ± 30.3 mL/min⻹/1.73 m⻲ and lowest in the DN subcohort. The overall prevalence of previous CVD was 14.4% in all patients, and was highest in the DN followed by that in the HTN subcohort. The DN subcohort had more adverse cardiovascular risk profiles (higher systolic blood pressure [SBP], and higher levels of cardiac troponin T, left ventricular mass index [LVMI], coronary calcium score, and brachial-ankle pulse wave velocity [baPWV]) than the other subcohorts. The HTN subcohort exhibited less severe cardiovascular risk profiles than the DN subcohort, but had more severe cardiovascular risk features than the GN and PKD subcohorts. All these cardiovascular risk profiles were inversely correlated with eGFR. In conclusion, this study shows that the KNOW-CKD cohort exhibits high cardiovascular burden, as other CKD cohorts in previous studies. Among the subcohorts, the DN subcohort had the highest risk for CVD. The ongoing long-term follow-up study up to 10 years will further delineate cardiovascular characteristics and outcomes of each subcohort exposed to different risk profiles.
Keyword
MeSH Terms
-
Adult*
Blood Pressure
Calcium
Cardiovascular Diseases
Cause of Death
Cohort Studies*
Diabetic Nephropathies
Epidemiology
Follow-Up Studies
Glomerular Filtration Rate
Glomerulonephritis
Humans
Hypertension
Polycystic Kidney Diseases
Prevalence
Pulse Wave Analysis
Renal Insufficiency, Chronic*
Troponin T
Calcium
Troponin T
Figure
-
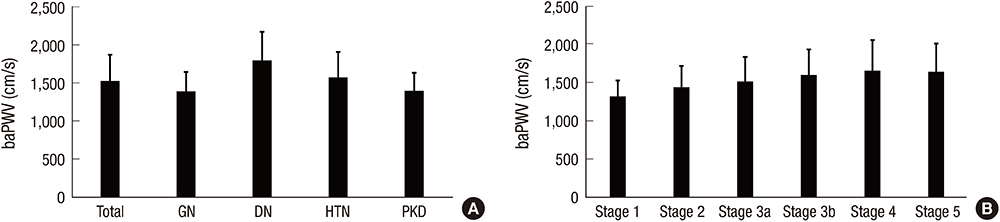
Fig. 1 baPWV of the participants. (A) baPWV according to the etiology of CKD. (B) baPWV according to the CKD stages. baPWV = brachial-ankle pulse wave velocity, CKD = chronic kidney disease, GN = glomerulonephritis, DN = diabetic nephropathy, HTN = hypertensive nephropathy, PKD = polycystic kidney disease.

Fig. 2 Categories of CAC score in the participants. (A) CAC according to the etiology of CKD. (B) CAC according to CKD stages. CAC = coronary arterial calcium, CKD = chronic kidney disease, GN = glomerulonephritis, DN = diabetic nephropathy, HTN = hypertensive nephropathy, PKD = polycystic kidney disease.
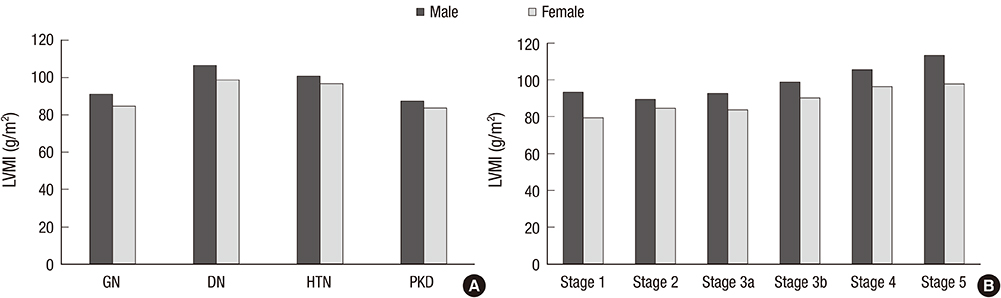
Fig. 3 LVMI of the participants. (A) LVMI according to the etiology of CKD. (B) LVMI according to CKD stages. LVMI = left ventricular mass index, CKD = chronic kidney disease, GN = glomerulonephritis, DN = diabetic nephropathy, HTN = hypertensive nephropathy, PKD = polycystic kidney disease.
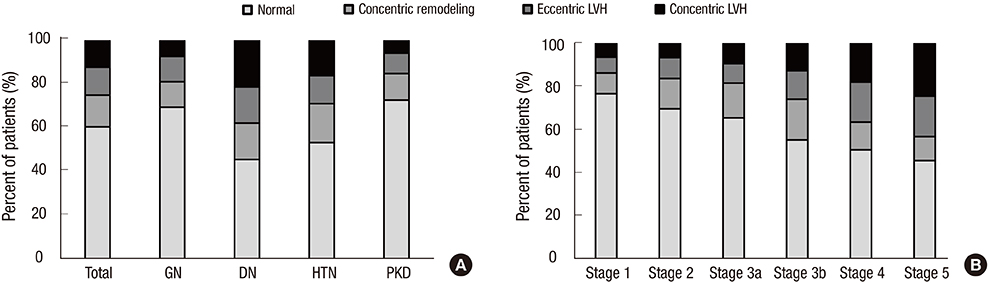
Fig. 4 LV geometry of the participants. (A) LV geometry according to the etiology of CKD. (B) LV geometry according to CKD stages. LV = Left ventricular, CKD = chronic kidney disease, GN = glomerulonephritis, DN = diabetic nephropathy, HTN = hypertensive nephropathy, PKD = polycystic kidney disease.
Reference
-
1. Jin DC. Major changes and improvements of dialysis therapy in Korea: review of end-stage renal disease registry. Korean J Intern Med. 2015; 30:17–22.2. Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS. Prevalence of chronic kidney disease in the United States. JAMA. 2007; 298:2038–2047.3. Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S, Hallan HA, Lydersen S, Holmen J. International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol. 2006; 17:2275–2284.4. Arora P, Vasa P, Brenner D, Iglar K, McFarlane P, Morrison H, Badawi A. Prevalence estimates of chronic kidney disease in Canada: results of a nationally representative survey. CMAJ. 2013; 185:E417–23.5. Imai E, Horio M, Watanabe T, Iseki K, Yamagata K, Hara S, Ura N, Kiyohara Y, Moriyama T, Ando Y, et al. Prevalence of chronic kidney disease in the Japanese general population. Clin Exp Nephrol. 2009; 13:621–630.6. Park JI, Baek H, Jung HH. Prevalence of chronic kidney disease in Korea: the Korean National Health and Nutritional Examination Survey 2011-2013. J Korean Med Sci. 2016; 31:915–923.7. Kim S, Lim CS, Han DC, Kim GS, Chin HJ, Kim SJ, Cho WY, Kim YH, Kim YS. The prevalence of chronic kidney disease (CKD) and the associated factors to CKD in urban Korea: a population-based cross-sectional epidemiologic study. J Korean Med Sci. 2009; 24:Suppl. S11–21.8. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004; 351:1296–1305.9. Shulman NB, Ford CE, Hall WD, Blaufox MD, Simon D, Langford HG, Schneider KA. Prognostic value of serum creatinine and effect of treatment of hypertension on renal function. Results from the hypertension detection and follow-up program. The Hypertension Detection and Follow-up Program Cooperative Group. Hypertension. 1989; 13:I80–93.10. Lash JP, Go AS, Appel LJ, He J, Ojo A, Rahman M, Townsend RR, Xie D, Cifelli D, Cohan J, et al. Chronic renal insufficiency cohort (CRIC) study: baseline characteristics and associations with kidney function. Clin J Am Soc Nephrol. 2009; 4:1302–1311.11. Ricardo AC, Lash JP, Fischer MJ, Lora CM, Budoff M, Keane MG, Kusek JW, Martinez M, Nessel L, Stamos T, et al. Cardiovascular disease among hispanics and non-hispanics in the chronic renal insufficiency cohort (CRIC) study. Clin J Am Soc Nephrol. 2011; 6:2121–2131.12. Mehrotra R, Kermah D, Fried L, Adler S, Norris K. Racial differences in mortality among those with CKD. J Am Soc Nephrol. 2008; 19:1403–1410.13. Rodriguez CJ, Sciacca RR, Diez-Roux AV, Boden-Albala B, Sacco RL, Homma S, DiTullio MR. Relation between socioeconomic status, race-ethnicity, and left ventricular mass: the Northern Manhattan study. Hypertension. 2004; 43:775–779.14. Gutiérrez OM, Anderson C, Isakova T, Scialla J, Negrea L, Anderson AH, Bellovich K, Chen J, Robinson N, Ojo A, et al. Low socioeconomic status associates with higher serum phosphate irrespective of race. J Am Soc Nephrol. 2010; 21:1953–1960.15. Imai E, Matsuo S, Makino H, Watanabe T, Akizawa T, Nitta K, Iimuro S, Ohashi Y, Hishida A. Chronic kidney disease Japan cohort study: baseline characteristics and factors associated with causative diseases and renal function. Clin Exp Nephrol. 2010; 14:558–570.16. Stevens PE, Levin A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013; 158:825–830.17. Astor BC, Hallan SI, Miller ER 3rd, Yeung E, Coresh J. Glomerular filtration rate, albuminuria, and risk of cardiovascular and all-cause mortality in the US population. Am J Epidemiol. 2008; 167:1226–1234.18. Levey AS, de Jong PE, Coresh J, El Nahas M, Astor BC, Matsushita K, Gansevoort RT, Kasiske BL, Eckardt KU. The definition, classification, and prognosis of chronic kidney disease: a KDIGO controversies conference report. Kidney Int. 2011; 80:17–28.19. Oh KH, Park SK, Park HC, Chin HJ, Chae DW, Choi KH, Han SH, Yoo TH, Lee K, Kim YS, et al. KNOW-CKD (Korean cohort study for outcome in patients with chronic kidney disease): design and methods. BMC Nephrol. 2014; 15:80.20. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999; 130:461–470.21. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise J, et al. Recommendations for chamber quantification. Eur J Echocardiogr. 2006; 7:79–108.22. Wong JS, Port FK, Hulbert-Shearon TE, Carroll CE, Wolfe RA, Agodoa LY, Daugirdas JT. Survival advantage in Asian American end-stage renal disease patients. Kidney Int. 1999; 55:2515–2523.23. Goodkin DA, Bragg-Gresham JL, Koenig KG, Wolfe RA, Akiba T, Andreucci VE, Saito A, Rayner HC, Kurokawa K, Port FK, et al. Association of comorbid conditions and mortality in hemodialysis patients in Europe, Japan, and the United States: the dialysis outcomes and practice patterns study (DOPPS). J Am Soc Nephrol. 2003; 14:3270–3277.24. Afkarian M, Katz R, Bansal N, Correa A, Kestenbaum B, Himmelfarb J, de Boer IH, Young B. Diabetes, kidney disease, and cardiovascular outcomes in the Jackson Heart Study. Clin J Am Soc Nephrol. 2016; 11:1384–1391.25. Kim YJ, Lim MN, Lee DS. Trend analysis in the prevalence of type 2 diabetes according to risk factors among Korean adults: based on the 2001~2009 Korean National Health and Nutrition Examination Survey data. J Korean Acad Nurs. 2014; 44:743–750.26. Ahn JH, Yu JH, Ko SH, Kwon HS, Kim DJ, Kim JH, Kim CS, Song KH, Won JC, Lim S, et al. Prevalence and determinants of diabetic nephropathy in Korea: Korea national health and nutrition examination survey. Diabetes Metab J. 2014; 38:109–119.27. Chen SC, Chang JM, Liu WC, Tsai YC, Tsai JC, Hsu PC, Lin TH, Lin MY, Su HM, Hwang SJ, et al. Brachial-ankle pulse wave velocity and rate of renal function decline and mortality in chronic kidney disease. Clin J Am Soc Nephrol. 2011; 6:724–732.28. Aumann N, Baumeister SE, Werner A, Wallaschofski H, Hannemann A, Nauck M, Rettig R, Felix SB, Dörr M, Völzke H, et al. Inverse association of estimated cystatin C- and creatinine-based glomerular filtration rate with left ventricular mass: results from the study of health in pomerania. Int J Cardiol. 2013; 167:2786–2791.29. Budoff MJ, Rader DJ, Reilly MP, Mohler ER 3rd, Lash J, Yang W, Rosen L, Glenn M, Teal V, Feldman HI; CRIC Study Investigators. Relationship of estimated GFR and coronary artery calcification in the CRIC (chronic renal insufficiency cohort) study. Am J Kidney Dis. 2011; 58:519–526.30. Lillie JS, Liberson AS, Mix D, Schwarz KQ, Chandra A, Phillips DB, Day SW, Borkholder DA. Pulse wave velocity prediction and compliance assessment in elastic arterial segments. Cardiovasc Eng Technol. 2015; 6:49–58.31. Chen SC, Huang JC, Tsai YC, Chen LI, Su HM, Chang JM, Chen HC. Body mass index, left ventricular mass index and cardiovascular events in chronic kidney disease. Am J Med Sci. 2016; 351:91–96.32. Matsushita K, Sang Y, Ballew SH, Shlipak M, Katz R, Rosas SE, Peralta CA, Woodward M, Kramer HJ, Jacobs DR, et al. Subclinical atherosclerosis measures for cardiovascular prediction in CKD. J Am Soc Nephrol. 2015; 26:439–447.33. Helal I, Reed B, Mettler P, Mc Fann K, Tkachenko O, Yan XD, Schrier RW. Prevalence of cardiovascular events in patients with autosomal dominant polycystic kidney disease. Am J Nephrol. 2012; 36:362–370.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The KoreaN Cohort Study for Outcomes in Patients With Chronic Kidney Disease (KNOW-CKD): A Korean Chronic Kidney Disease Cohort
- Risk Factors for the Progression of Chronic Kidney Disease in Children
- Anemia in children with chronic kidney disease
- Osteoporosis in Patients with Chronic Kidney Disease
- Diagnosis and Management of Chronic Kidney Disease-Mineral Bone Disease in Children
